Manuel Giovanni Mazzoleni, Nicola Maffulli, Tommaso Bardazzi, Michael Memminger, Francesca Alzira Bertini, Filippo Migliorini
{"title":"尾骨神经痛的治疗:近期临床试验系统回顾的要点。","authors":"Manuel Giovanni Mazzoleni, Nicola Maffulli, Tommaso Bardazzi, Michael Memminger, Francesca Alzira Bertini, Filippo Migliorini","doi":"10.21037/aoj-24-40","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coccygodynia, characterised by localised pain in the coccyx and surrounding tissues, presents challenges in diagnosis and management given its low prevalence and varied aetiology. Traumatic injury, particularly backward falls, is commonly implicated, while non-traumatic causes include degenerative joint disease, overloading stress forces from obesity and morphological variations of the coccyx. Diagnostic evaluation involves medical history, physical examination, and radiographic imaging. While conservative management is often successful, refractory cases necessitate intervention. However, optimal treatment strategies still need to be clarified. The present systematic review discusses the clinical evidence on the management of coccygodynia.</p><p><strong>Methods: </strong>In December 2024, a systematic review followed PRISMA guidelines, accessing PubMed, Web of Science, and Embase databases. Eligible studies included solely clinical trials investigating coccygodynia management. The risk of bias was assessed using Cochrane risk of bias assessment tool (RoB2) for randomized controlled trials (RCTs) and the Risk of Bias in nonrandomized Studies of Interventions (ROBINS-I) for non-RCTs. Data extraction and statistical analyses followed the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions.</p><p><strong>Results: </strong>Of 407 identified articles, 16 met inclusion criteria, comprising 858 patients, primarily women. Risk of bias assessment revealed varying methodological quality among included studies. Conservative treatments, including physiotherapy and shockwave therapy, showed promise in pain management. Interventional therapies, such as corticosteroid injections and ganglion-impair blockade, demonstrated efficacy in refractory cases. Surgical interventions, particularly coccygectomy, yielded moderate success rates but were associated with notable risks.</p><p><strong>Conclusions: </strong>A multidisciplinary approach is advocated for managing coccygodynia, with conservative measures as initial strategies. Physical therapy-based interventions and interventional treatments, such as corticosteroid injections and ganglion impair blockade, offer viable options for refractory cases. Surgical intervention should be considered judiciously, weighing risks and benefits based on patient-specific factors and treatment response. Further research is needed to establish standardized guidelines for coccygodynia management based on high-quality evidence.</p>","PeriodicalId":44459,"journal":{"name":"Annals of Joint","volume":"10 ","pages":"9"},"PeriodicalIF":0.9000,"publicationDate":"2025-01-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11836747/pdf/","citationCount":"0","resultStr":"{\"title\":\"Management of coccygodynia: talking points from a systematic review of recent clinical trials.\",\"authors\":\"Manuel Giovanni Mazzoleni, Nicola Maffulli, Tommaso Bardazzi, Michael Memminger, Francesca Alzira Bertini, Filippo Migliorini\",\"doi\":\"10.21037/aoj-24-40\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Coccygodynia, characterised by localised pain in the coccyx and surrounding tissues, presents challenges in diagnosis and management given its low prevalence and varied aetiology. Traumatic injury, particularly backward falls, is commonly implicated, while non-traumatic causes include degenerative joint disease, overloading stress forces from obesity and morphological variations of the coccyx. Diagnostic evaluation involves medical history, physical examination, and radiographic imaging. While conservative management is often successful, refractory cases necessitate intervention. However, optimal treatment strategies still need to be clarified. The present systematic review discusses the clinical evidence on the management of coccygodynia.</p><p><strong>Methods: </strong>In December 2024, a systematic review followed PRISMA guidelines, accessing PubMed, Web of Science, and Embase databases. Eligible studies included solely clinical trials investigating coccygodynia management. The risk of bias was assessed using Cochrane risk of bias assessment tool (RoB2) for randomized controlled trials (RCTs) and the Risk of Bias in nonrandomized Studies of Interventions (ROBINS-I) for non-RCTs. Data extraction and statistical analyses followed the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions.</p><p><strong>Results: </strong>Of 407 identified articles, 16 met inclusion criteria, comprising 858 patients, primarily women. Risk of bias assessment revealed varying methodological quality among included studies. Conservative treatments, including physiotherapy and shockwave therapy, showed promise in pain management. Interventional therapies, such as corticosteroid injections and ganglion-impair blockade, demonstrated efficacy in refractory cases. Surgical interventions, particularly coccygectomy, yielded moderate success rates but were associated with notable risks.</p><p><strong>Conclusions: </strong>A multidisciplinary approach is advocated for managing coccygodynia, with conservative measures as initial strategies. Physical therapy-based interventions and interventional treatments, such as corticosteroid injections and ganglion impair blockade, offer viable options for refractory cases. Surgical intervention should be considered judiciously, weighing risks and benefits based on patient-specific factors and treatment response. Further research is needed to establish standardized guidelines for coccygodynia management based on high-quality evidence.</p>\",\"PeriodicalId\":44459,\"journal\":{\"name\":\"Annals of Joint\",\"volume\":\"10 \",\"pages\":\"9\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-01-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11836747/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Joint\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/aoj-24-40\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Joint","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/aoj-24-40","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:尾骨痛的特点是尾骨和周围组织的局部疼痛,由于其低患病率和多种病因,在诊断和治疗方面提出了挑战。通常涉及外伤性损伤,特别是向后跌倒,而非外伤性原因包括退行性关节疾病、肥胖造成的过度应力和尾骨形态变化。诊断评估包括病史、体格检查和放射影像。虽然保守治疗通常是成功的,但难治性病例需要干预。然而,最佳治疗策略仍需明确。本系统综述讨论了治疗尾骨痛的临床证据。方法:2024年12月,遵循PRISMA指南,访问PubMed、Web of Science和Embase数据库,进行系统评价。符合条件的研究包括调查尾骨痛治疗的单独临床试验。随机对照试验(rct)采用Cochrane偏倚风险评估工具(RoB2)评估偏倚风险,非随机对照试验采用非随机干预研究(ROBINS-I)评估偏倚风险。数据提取和统计分析遵循Cochrane干预措施系统评价手册的建议。结果:在407篇确定的文章中,16篇符合纳入标准,包括858例患者,主要是女性。偏倚风险评估显示纳入研究的方法学质量存在差异。包括物理疗法和冲击波疗法在内的保守疗法在疼痛管理方面显示出希望。介入治疗,如皮质类固醇注射和神经节损伤阻断,对难治性病例有效。手术干预,特别是尾骨切除术,取得了中等的成功率,但与显著的风险相关。结论:提倡多学科方法治疗尾骨痛,以保守措施为初始策略。以物理治疗为基础的干预和介入治疗,如皮质类固醇注射和神经节损伤阻断,为难治性病例提供了可行的选择。手术干预应审慎考虑,根据患者的具体因素和治疗反应权衡风险和收益。需要进一步的研究来建立基于高质量证据的尾骨痛管理的标准化指南。
Management of coccygodynia: talking points from a systematic review of recent clinical trials.
Background: Coccygodynia, characterised by localised pain in the coccyx and surrounding tissues, presents challenges in diagnosis and management given its low prevalence and varied aetiology. Traumatic injury, particularly backward falls, is commonly implicated, while non-traumatic causes include degenerative joint disease, overloading stress forces from obesity and morphological variations of the coccyx. Diagnostic evaluation involves medical history, physical examination, and radiographic imaging. While conservative management is often successful, refractory cases necessitate intervention. However, optimal treatment strategies still need to be clarified. The present systematic review discusses the clinical evidence on the management of coccygodynia.
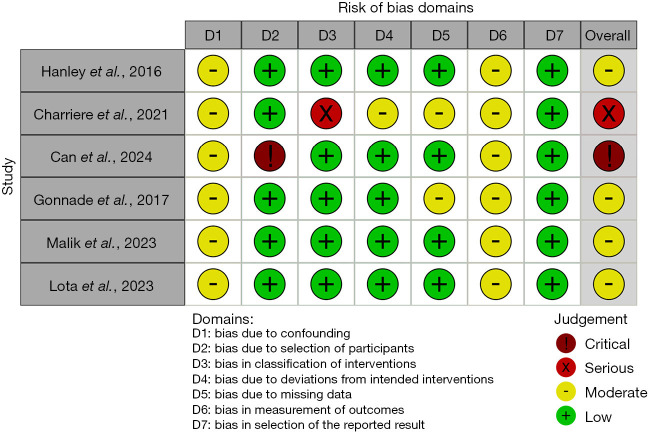
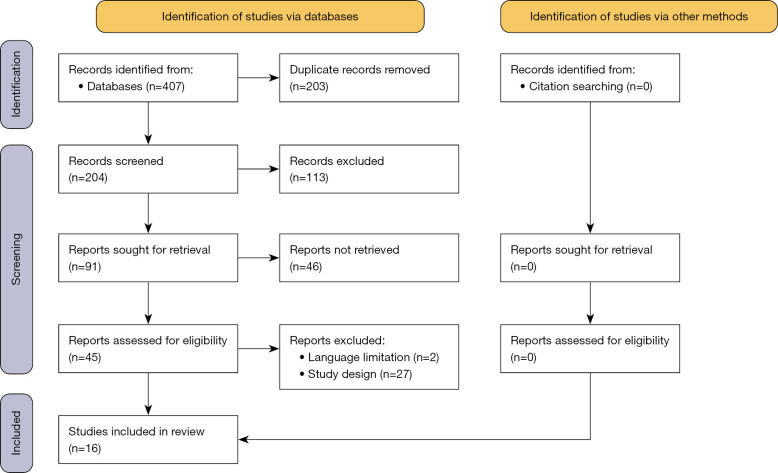
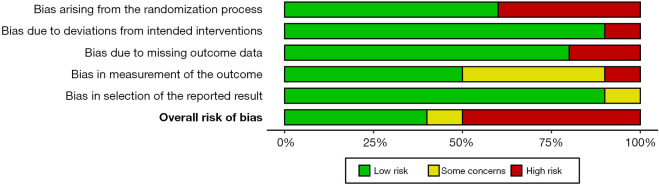
Methods: In December 2024, a systematic review followed PRISMA guidelines, accessing PubMed, Web of Science, and Embase databases. Eligible studies included solely clinical trials investigating coccygodynia management. The risk of bias was assessed using Cochrane risk of bias assessment tool (RoB2) for randomized controlled trials (RCTs) and the Risk of Bias in nonrandomized Studies of Interventions (ROBINS-I) for non-RCTs. Data extraction and statistical analyses followed the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions.
Results: Of 407 identified articles, 16 met inclusion criteria, comprising 858 patients, primarily women. Risk of bias assessment revealed varying methodological quality among included studies. Conservative treatments, including physiotherapy and shockwave therapy, showed promise in pain management. Interventional therapies, such as corticosteroid injections and ganglion-impair blockade, demonstrated efficacy in refractory cases. Surgical interventions, particularly coccygectomy, yielded moderate success rates but were associated with notable risks.
Conclusions: A multidisciplinary approach is advocated for managing coccygodynia, with conservative measures as initial strategies. Physical therapy-based interventions and interventional treatments, such as corticosteroid injections and ganglion impair blockade, offer viable options for refractory cases. Surgical intervention should be considered judiciously, weighing risks and benefits based on patient-specific factors and treatment response. Further research is needed to establish standardized guidelines for coccygodynia management based on high-quality evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


