{"title":"质量改进合作增加剖腹产的可及性:来自印度比哈尔邦的经验。","authors":"Abha Mehndiratta, Prabir Ranjan Moharana, Tanmay Mahapatra, Sridhar Srikantiah, Sunil Babu, Sarita Simba, Sanjiv Daulatrao, Vikas Pandey, Rahul Shastri, Srinivas Kodiyath, Sulagna Mukherjee, Pramod Sah, Pierre Barker","doi":"10.1136/bmjqs-2024-017454","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Countries with resource-poor health systems have struggled to improve access to and the quality of caesarean section (C-section; CS) for women seeking care in public health facilities. Access to C-section in Bihar State remains very low, while access has increased in many other contexts.</p><p><strong>Methods: </strong>We used quality improvement (QI) combined with targeted resource management to test and implement changes that were designed to increase C-section delivery. We compared C-section delivery percentages after the interventions across eight intervened (QI) hospitals and between QI hospitals and the remaining 22 non-intervened (non-QI) hospitals with baseline CS <10%. We linked patterns of improvement and sustainability to theoretical drivers of improvement and timing of interventions.</p><p><strong>Results: </strong>In QI hospitals, C-section percentage increased from 2.9% at baseline to 5.9% in the intervention phase and 4.6% in the post intervention phase. In non-QI hospitals, we observed a small change (2.6-3.3%) during the same time period of the interventions in the QI hospitals. Addition of skilled personnel resulted in increased C-section percentage in QI hospitals (3.6-5.9%) but not non-QI hospitals (3.4-3.2%).</p><p><strong>Conclusions: </strong>C-section availability increased for a population of women giving birth following initiation of QI BTS collaborative in a low-income country public sector setting that has historically struggled to provide this service. Addition of obstetric and operating room resources alone, without interventions to support system changes, may not result in additional increase in C-section delivery. The adaptive implementation model may contribute to efforts to provide more access to C-sections in other very resource-limited settings.</p>","PeriodicalId":9077,"journal":{"name":"BMJ Quality & Safety","volume":" ","pages":"404-412"},"PeriodicalIF":6.5000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12171458/pdf/","citationCount":"0","resultStr":"{\"title\":\"Quality improvement collaborative to increase access to caesarean sections: lessons from Bihar, India.\",\"authors\":\"Abha Mehndiratta, Prabir Ranjan Moharana, Tanmay Mahapatra, Sridhar Srikantiah, Sunil Babu, Sarita Simba, Sanjiv Daulatrao, Vikas Pandey, Rahul Shastri, Srinivas Kodiyath, Sulagna Mukherjee, Pramod Sah, Pierre Barker\",\"doi\":\"10.1136/bmjqs-2024-017454\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Countries with resource-poor health systems have struggled to improve access to and the quality of caesarean section (C-section; CS) for women seeking care in public health facilities. Access to C-section in Bihar State remains very low, while access has increased in many other contexts.</p><p><strong>Methods: </strong>We used quality improvement (QI) combined with targeted resource management to test and implement changes that were designed to increase C-section delivery. We compared C-section delivery percentages after the interventions across eight intervened (QI) hospitals and between QI hospitals and the remaining 22 non-intervened (non-QI) hospitals with baseline CS <10%. We linked patterns of improvement and sustainability to theoretical drivers of improvement and timing of interventions.</p><p><strong>Results: </strong>In QI hospitals, C-section percentage increased from 2.9% at baseline to 5.9% in the intervention phase and 4.6% in the post intervention phase. In non-QI hospitals, we observed a small change (2.6-3.3%) during the same time period of the interventions in the QI hospitals. Addition of skilled personnel resulted in increased C-section percentage in QI hospitals (3.6-5.9%) but not non-QI hospitals (3.4-3.2%).</p><p><strong>Conclusions: </strong>C-section availability increased for a population of women giving birth following initiation of QI BTS collaborative in a low-income country public sector setting that has historically struggled to provide this service. Addition of obstetric and operating room resources alone, without interventions to support system changes, may not result in additional increase in C-section delivery. The adaptive implementation model may contribute to efforts to provide more access to C-sections in other very resource-limited settings.</p>\",\"PeriodicalId\":9077,\"journal\":{\"name\":\"BMJ Quality & Safety\",\"volume\":\" \",\"pages\":\"404-412\"},\"PeriodicalIF\":6.5000,\"publicationDate\":\"2025-05-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12171458/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Quality & Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjqs-2024-017454\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Quality & Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjqs-2024-017454","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Quality improvement collaborative to increase access to caesarean sections: lessons from Bihar, India.
Background: Countries with resource-poor health systems have struggled to improve access to and the quality of caesarean section (C-section; CS) for women seeking care in public health facilities. Access to C-section in Bihar State remains very low, while access has increased in many other contexts.
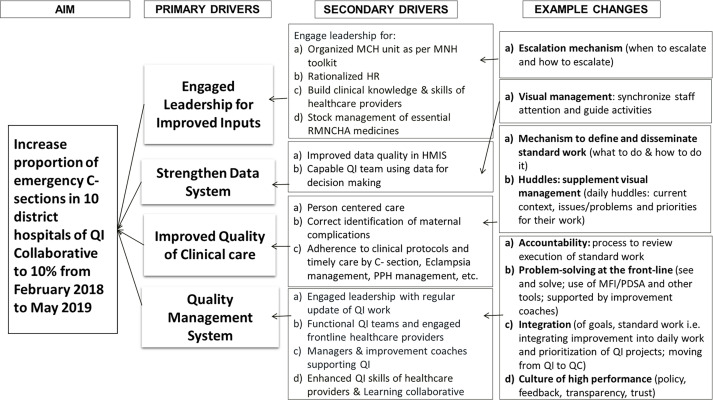
Methods: We used quality improvement (QI) combined with targeted resource management to test and implement changes that were designed to increase C-section delivery. We compared C-section delivery percentages after the interventions across eight intervened (QI) hospitals and between QI hospitals and the remaining 22 non-intervened (non-QI) hospitals with baseline CS <10%. We linked patterns of improvement and sustainability to theoretical drivers of improvement and timing of interventions.
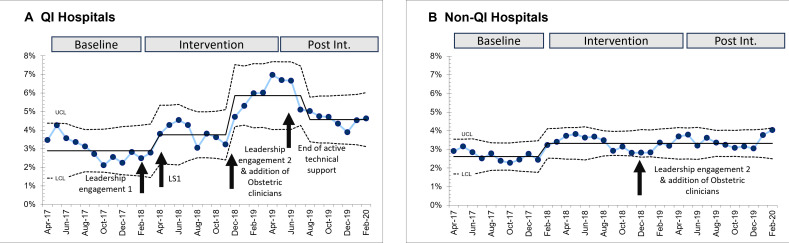
Results: In QI hospitals, C-section percentage increased from 2.9% at baseline to 5.9% in the intervention phase and 4.6% in the post intervention phase. In non-QI hospitals, we observed a small change (2.6-3.3%) during the same time period of the interventions in the QI hospitals. Addition of skilled personnel resulted in increased C-section percentage in QI hospitals (3.6-5.9%) but not non-QI hospitals (3.4-3.2%).
Conclusions: C-section availability increased for a population of women giving birth following initiation of QI BTS collaborative in a low-income country public sector setting that has historically struggled to provide this service. Addition of obstetric and operating room resources alone, without interventions to support system changes, may not result in additional increase in C-section delivery. The adaptive implementation model may contribute to efforts to provide more access to C-sections in other very resource-limited settings.
期刊介绍:
BMJ Quality & Safety (previously Quality & Safety in Health Care) is an international peer review publication providing research, opinions, debates and reviews for academics, clinicians and healthcare managers focused on the quality and safety of health care and the science of improvement.
The journal receives approximately 1000 manuscripts a year and has an acceptance rate for original research of 12%. Time from submission to first decision averages 22 days and accepted articles are typically published online within 20 days. Its current impact factor is 3.281.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


