Pruthvi C Revaiah, Kotaro Miyashita, Tsung-Ying Tsai, Retesh Bajaj, Nozomi Kotoku, Akihiro Tobe, Takashi Muramatsu, Kengo Tanabe, Ken Kozuma, Yukio Ozaki, Scot Garg, Shengxian Tu, Jouke Dijkstra, Christos V Bourantas, Yoshinobu Onuma, Patrick W Serruys
{"title":"经皮冠状动脉介入治疗后的超声或光流比分段生理梯度:来自ASET JAPAN研究的见解。","authors":"Pruthvi C Revaiah, Kotaro Miyashita, Tsung-Ying Tsai, Retesh Bajaj, Nozomi Kotoku, Akihiro Tobe, Takashi Muramatsu, Kengo Tanabe, Ken Kozuma, Yukio Ozaki, Scot Garg, Shengxian Tu, Jouke Dijkstra, Christos V Bourantas, Yoshinobu Onuma, Patrick W Serruys","doi":"10.1093/ehjimp/qyaf017","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Segmental pressure gradients post-percutaneous coronary intervention (PCI) can detect residual disease and optimization targets. Ultrasonic flow ratio (UFR) or optical flow ratio (OFR) offer simultaneous physiological and morphological assessment using a single imaging catheter. This study evaluated the utility of UFR and OFR in identifying residual disease post-PCI.</p><p><strong>Methods and results: </strong>The study include patients from the Acetyl Salicylic Elimination Trial JAPAN Pilot study with complete intravascular imaging pullback data, where UFR or OFR was obtained post-PCI. Anatomical focal lesions distal and proximal to the stent were analysed in segments ≥5 mm long. UFR or OFR virtual pullback curves assessed intra-stent pressure gradients, defining physiological focal or diffuse by segmental pressure drops ≥0.05 over lengths <10 or ≥10 mm, respectively. The median post-PCI UFR/OFR was 0.93 (0.88-0.96) with 35.4% (69/195) vessels having a UFR/OFR < 0.91. There were significantly more focal lesions, both anatomical and physiological, proximal and distal to the stent in vessels with UFR/OFR < 0.91 compared with those ≥0.91. Agreement between anatomical and physiological focal lesions was moderate proximally (kappa = 0.553, <i>P</i> < 0.001) and fair distally (kappa = 0.219, <i>P</i> = 0.002). The in-stent gradient poorly predicted significant stent under-expansion. However, the virtual fractional flow reserve gradient performed well in detecting proximal or distal focal disease (area under the curve = 0.835 and 0.877, respectively).</p><p><strong>Conclusion: </strong>UFR/OFR effectively identifies sub-optimal vessel physiology post-PCI and locates precise anatomical issues, validated by intravascular imaging.</p><p><strong>Trial registration: </strong>The ASET JAPAN ClinicalTrials.gov reference: NCT05117866.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"3 1","pages":"qyaf017"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11837184/pdf/","citationCount":"0","resultStr":"{\"title\":\"Segmental post-percutaneous coronary intervention physiological gradients using ultrasonic or optical flow ratio: insights from ASET JAPAN study.\",\"authors\":\"Pruthvi C Revaiah, Kotaro Miyashita, Tsung-Ying Tsai, Retesh Bajaj, Nozomi Kotoku, Akihiro Tobe, Takashi Muramatsu, Kengo Tanabe, Ken Kozuma, Yukio Ozaki, Scot Garg, Shengxian Tu, Jouke Dijkstra, Christos V Bourantas, Yoshinobu Onuma, Patrick W Serruys\",\"doi\":\"10.1093/ehjimp/qyaf017\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Segmental pressure gradients post-percutaneous coronary intervention (PCI) can detect residual disease and optimization targets. Ultrasonic flow ratio (UFR) or optical flow ratio (OFR) offer simultaneous physiological and morphological assessment using a single imaging catheter. This study evaluated the utility of UFR and OFR in identifying residual disease post-PCI.</p><p><strong>Methods and results: </strong>The study include patients from the Acetyl Salicylic Elimination Trial JAPAN Pilot study with complete intravascular imaging pullback data, where UFR or OFR was obtained post-PCI. Anatomical focal lesions distal and proximal to the stent were analysed in segments ≥5 mm long. UFR or OFR virtual pullback curves assessed intra-stent pressure gradients, defining physiological focal or diffuse by segmental pressure drops ≥0.05 over lengths <10 or ≥10 mm, respectively. The median post-PCI UFR/OFR was 0.93 (0.88-0.96) with 35.4% (69/195) vessels having a UFR/OFR < 0.91. There were significantly more focal lesions, both anatomical and physiological, proximal and distal to the stent in vessels with UFR/OFR < 0.91 compared with those ≥0.91. Agreement between anatomical and physiological focal lesions was moderate proximally (kappa = 0.553, <i>P</i> < 0.001) and fair distally (kappa = 0.219, <i>P</i> = 0.002). The in-stent gradient poorly predicted significant stent under-expansion. However, the virtual fractional flow reserve gradient performed well in detecting proximal or distal focal disease (area under the curve = 0.835 and 0.877, respectively).</p><p><strong>Conclusion: </strong>UFR/OFR effectively identifies sub-optimal vessel physiology post-PCI and locates precise anatomical issues, validated by intravascular imaging.</p><p><strong>Trial registration: </strong>The ASET JAPAN ClinicalTrials.gov reference: NCT05117866.</p>\",\"PeriodicalId\":94317,\"journal\":{\"name\":\"European heart journal. Imaging methods and practice\",\"volume\":\"3 1\",\"pages\":\"qyaf017\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-01-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11837184/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Imaging methods and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjimp/qyaf017\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:经皮冠状动脉介入治疗(PCI)后节段压力梯度检测残留病变及优化靶点。超声流量比(UFR)或光流量比(OFR)使用单个成像导管提供同时的生理和形态评估。本研究评估了UFR和OFR在pci术后残留病变识别中的应用。方法和结果:该研究包括来自乙酰水杨酸消除试验日本试点研究的患者,具有完整的血管内成像回拉数据,其中UFR或OFR在pci后获得。解剖局灶病变的远端和近端分析≥5mm长的节段。UFR或OFR虚拟回拉曲线评估支架内压力梯度,通过节段压降(≥0.05,P < 0.001)和远端压降(kappa = 0.219, P = 0.002)定义生理局灶性或弥漫性。支架内梯度难以预测显著的支架欠扩张。然而,虚拟分数流量储备梯度在检测近端或远端局灶性疾病方面表现良好(曲线下面积分别为0.835和0.877)。结论:UFR/OFR可以有效识别pci后的次优血管生理,并通过血管内成像验证精确定位解剖问题。试验注册:ASET JAPAN ClinicalTrials.gov参考:NCT05117866。
Segmental post-percutaneous coronary intervention physiological gradients using ultrasonic or optical flow ratio: insights from ASET JAPAN study.
Aims: Segmental pressure gradients post-percutaneous coronary intervention (PCI) can detect residual disease and optimization targets. Ultrasonic flow ratio (UFR) or optical flow ratio (OFR) offer simultaneous physiological and morphological assessment using a single imaging catheter. This study evaluated the utility of UFR and OFR in identifying residual disease post-PCI.
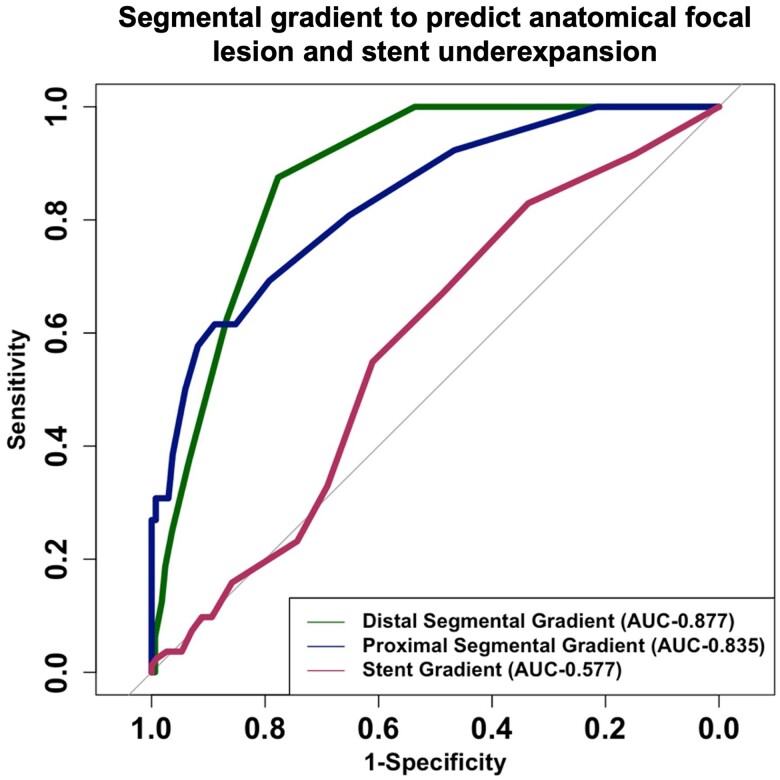
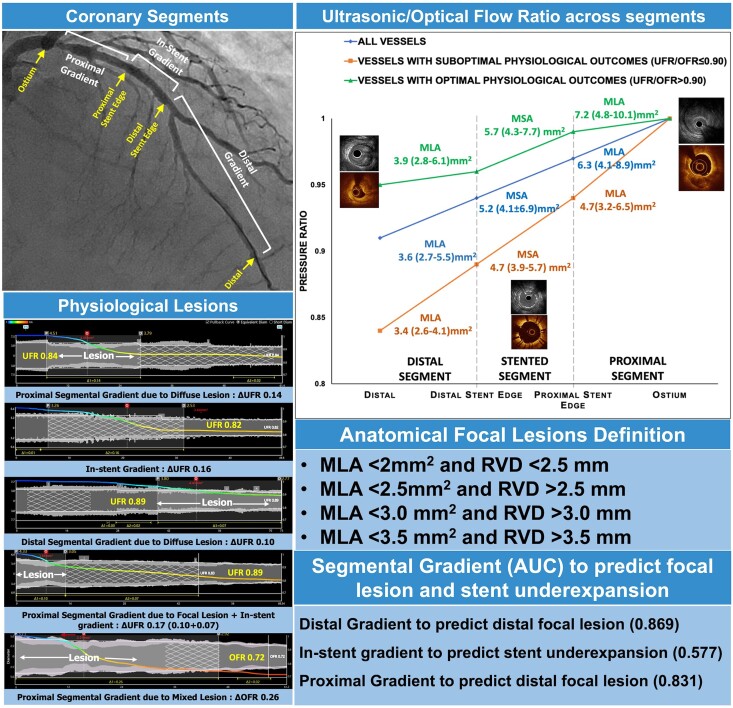
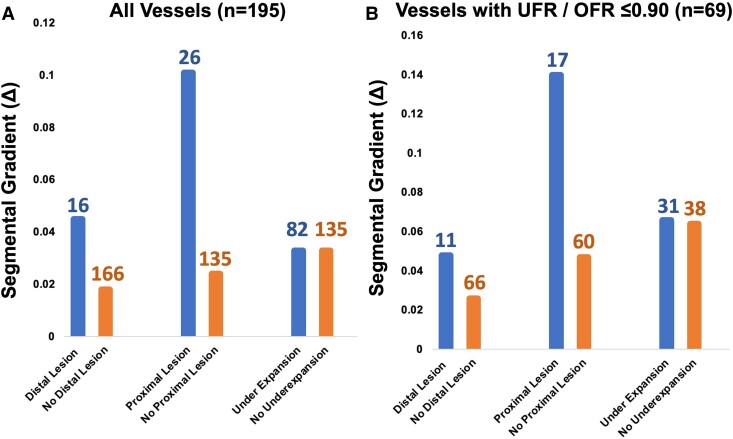
Methods and results: The study include patients from the Acetyl Salicylic Elimination Trial JAPAN Pilot study with complete intravascular imaging pullback data, where UFR or OFR was obtained post-PCI. Anatomical focal lesions distal and proximal to the stent were analysed in segments ≥5 mm long. UFR or OFR virtual pullback curves assessed intra-stent pressure gradients, defining physiological focal or diffuse by segmental pressure drops ≥0.05 over lengths <10 or ≥10 mm, respectively. The median post-PCI UFR/OFR was 0.93 (0.88-0.96) with 35.4% (69/195) vessels having a UFR/OFR < 0.91. There were significantly more focal lesions, both anatomical and physiological, proximal and distal to the stent in vessels with UFR/OFR < 0.91 compared with those ≥0.91. Agreement between anatomical and physiological focal lesions was moderate proximally (kappa = 0.553, P < 0.001) and fair distally (kappa = 0.219, P = 0.002). The in-stent gradient poorly predicted significant stent under-expansion. However, the virtual fractional flow reserve gradient performed well in detecting proximal or distal focal disease (area under the curve = 0.835 and 0.877, respectively).
Conclusion: UFR/OFR effectively identifies sub-optimal vessel physiology post-PCI and locates precise anatomical issues, validated by intravascular imaging.
Trial registration: The ASET JAPAN ClinicalTrials.gov reference: NCT05117866.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


