Madison Riccardi, Robert Contento, Cory Christensen, Amy Brady, Rebecca L Swan, Robert T Swan
{"title":"乳房x光检查诊断结节性葡萄膜炎1例。","authors":"Madison Riccardi, Robert Contento, Cory Christensen, Amy Brady, Rebecca L Swan, Robert T Swan","doi":"10.1155/crop/8871004","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose:</b> Sarcoidosis is a systemic inflammatory disease associated with ocular involvement in 20%-30% of cases. The current gold standard for detecting sarcoidosis is computed tomography of the thorax, which is 73% sensitive. Definitive diagnosis necessitates biopsy, with Schaumann bodies and non-necrotizing granulomas serving as key pathological hallmarks. <b>Observations:</b> Our patient, a 44-year-old White female, presented for a second opinion on her bilateral chronic intermediate uveitis with intractable chronic cystoid macular edema of the left eye. Our clinical suspicion for sarcoidosis was high, but the computed tomography thorax scan did not show any abnormal findings. A routine mammogram completed 4 weeks prior to our initial evaluation showed axillary lymph node enlargement with calcifications. Subsequent biopsy was consistent with sarcoidosis. Treatment with mycophenolate mofetil resolved the uveitis and macular edema. <b>Conclusions and Importance:</b> The diagnosis of sarcoidosis can be challenging due to nonspecific ocular signs and the potential for falsely negative findings on imaging. This case highlights the importance of patient education and self-surveillance regarding the characteristic systemic symptoms of sarcoidosis, which commonly involve the lungs, eyes, skin, joints, etc. Our report demonstrates the significance of maintaining a high level of suspicion for sarcoidosis in patients with characteristic ocular findings, even when initial imaging results are negative or inconclusive.</p>","PeriodicalId":9603,"journal":{"name":"Case Reports in Ophthalmological Medicine","volume":"2025 ","pages":"8871004"},"PeriodicalIF":0.4000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11839256/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Case of Sarcoid Uveitis Diagnosed With Mammography Two Months After Normal Chest Imaging.\",\"authors\":\"Madison Riccardi, Robert Contento, Cory Christensen, Amy Brady, Rebecca L Swan, Robert T Swan\",\"doi\":\"10.1155/crop/8871004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Purpose:</b> Sarcoidosis is a systemic inflammatory disease associated with ocular involvement in 20%-30% of cases. The current gold standard for detecting sarcoidosis is computed tomography of the thorax, which is 73% sensitive. Definitive diagnosis necessitates biopsy, with Schaumann bodies and non-necrotizing granulomas serving as key pathological hallmarks. <b>Observations:</b> Our patient, a 44-year-old White female, presented for a second opinion on her bilateral chronic intermediate uveitis with intractable chronic cystoid macular edema of the left eye. Our clinical suspicion for sarcoidosis was high, but the computed tomography thorax scan did not show any abnormal findings. A routine mammogram completed 4 weeks prior to our initial evaluation showed axillary lymph node enlargement with calcifications. Subsequent biopsy was consistent with sarcoidosis. Treatment with mycophenolate mofetil resolved the uveitis and macular edema. <b>Conclusions and Importance:</b> The diagnosis of sarcoidosis can be challenging due to nonspecific ocular signs and the potential for falsely negative findings on imaging. This case highlights the importance of patient education and self-surveillance regarding the characteristic systemic symptoms of sarcoidosis, which commonly involve the lungs, eyes, skin, joints, etc. Our report demonstrates the significance of maintaining a high level of suspicion for sarcoidosis in patients with characteristic ocular findings, even when initial imaging results are negative or inconclusive.</p>\",\"PeriodicalId\":9603,\"journal\":{\"name\":\"Case Reports in Ophthalmological Medicine\",\"volume\":\"2025 \",\"pages\":\"8871004\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2025-02-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11839256/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Ophthalmological Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crop/8871004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"OPHTHALMOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Ophthalmological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crop/8871004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
A Case of Sarcoid Uveitis Diagnosed With Mammography Two Months After Normal Chest Imaging.
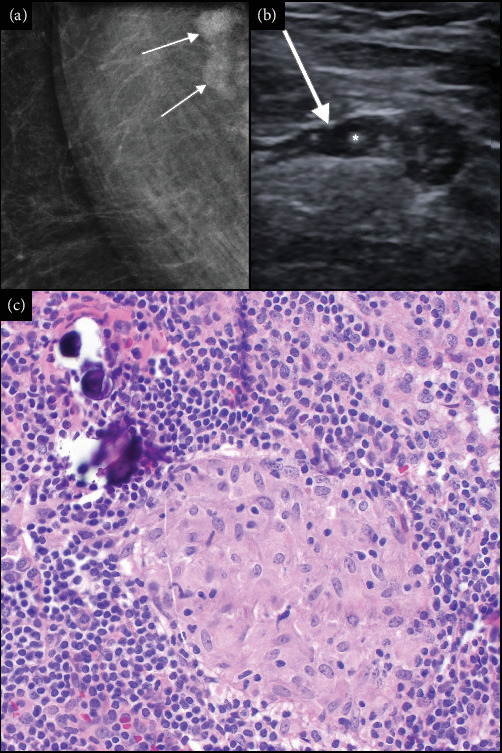
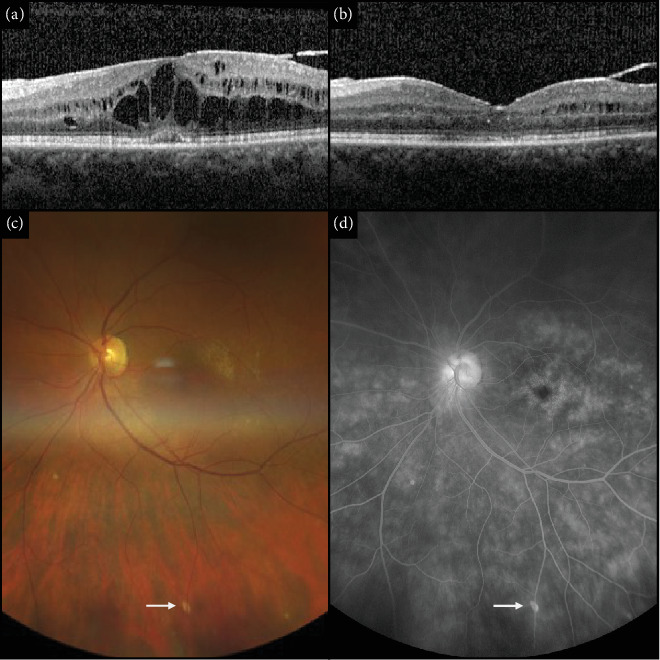
Purpose: Sarcoidosis is a systemic inflammatory disease associated with ocular involvement in 20%-30% of cases. The current gold standard for detecting sarcoidosis is computed tomography of the thorax, which is 73% sensitive. Definitive diagnosis necessitates biopsy, with Schaumann bodies and non-necrotizing granulomas serving as key pathological hallmarks. Observations: Our patient, a 44-year-old White female, presented for a second opinion on her bilateral chronic intermediate uveitis with intractable chronic cystoid macular edema of the left eye. Our clinical suspicion for sarcoidosis was high, but the computed tomography thorax scan did not show any abnormal findings. A routine mammogram completed 4 weeks prior to our initial evaluation showed axillary lymph node enlargement with calcifications. Subsequent biopsy was consistent with sarcoidosis. Treatment with mycophenolate mofetil resolved the uveitis and macular edema. Conclusions and Importance: The diagnosis of sarcoidosis can be challenging due to nonspecific ocular signs and the potential for falsely negative findings on imaging. This case highlights the importance of patient education and self-surveillance regarding the characteristic systemic symptoms of sarcoidosis, which commonly involve the lungs, eyes, skin, joints, etc. Our report demonstrates the significance of maintaining a high level of suspicion for sarcoidosis in patients with characteristic ocular findings, even when initial imaging results are negative or inconclusive.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


