Roni Bitterman, Hafid Soualhine, Pierre-Marie Akochy, Charles Poirier, Pasquale Ferraro, Dima Kabbani, Alim Hirji, Gregory Tyrrell, Celine Bergeron, Robert D Levy, Alissa Wright, Victor Leung, Lianne G Singer, Cecilia Chaparro, Shaf Keshavjee, Melissa Richard-Greenblatt, Shahid Husain, Me-Linh Luong
{"title":"肺移植受者并发脓肿分枝杆菌感染:加拿大一项多中心回顾性队列研究","authors":"Roni Bitterman, Hafid Soualhine, Pierre-Marie Akochy, Charles Poirier, Pasquale Ferraro, Dima Kabbani, Alim Hirji, Gregory Tyrrell, Celine Bergeron, Robert D Levy, Alissa Wright, Victor Leung, Lianne G Singer, Cecilia Chaparro, Shaf Keshavjee, Melissa Richard-Greenblatt, Shahid Husain, Me-Linh Luong","doi":"10.1111/tid.70003","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mycobacterium abscessus complex is known to cause life-threatening disease in lung transplantation (LT) recipients (LTRs). Therefore, many centers consider the presence of M. abscessus as a relative contraindication to LT.</p><p><strong>Methods: </strong>We conducted a multicenter retrospective cohort study including all 4 LT centers in Canada. All LTRs transplanted in 2006-2016 with at least one respiratory sample positive for M. abscessus prior or posttransplantation were included. Pulmonary disease was defined using the American Thoracic Society criteria. Minimal follow-up duration was 5 years after transplantation.</p><p><strong>Results: </strong>Among 2181 LTRs across Canada, 14 had M. abscessus disease after LT (incidence rate 1.1/1000 transplant-years) and 6 had pulmonary colonization (incidence rate 0.5/1000 transplant-years). Fifteen patients had M. abscessus cultured before LT. Among those with pretransplant M. abscessus, 53% (8/15) developed M. abscessus infection posttransplant (6 disease, 2 colonization). Posttransplant disease was less frequent among those with microbiologic eradication before transplant (0% vs. 85.7%, p = 0.001). LTRs with pretransplant M. abscessus had comparable survival to those without M. abscessus (log rank p = 0.37). Among patients with pretransplant infection, mortality was higher in those who did not achieve microbiological eradication before transplantation (57.1% vs. 0%, p = 0.03) and those who developed disease after transplantation (66.7% vs. 0%, p = 0.01).</p><p><strong>Conclusions: </strong>M. abscessus is an uncommon cause of infection among LTRs. Survival among those with pretransplant M. abscessus infection was similar to that observed in noninfected LTRs. However, lack of eradication before transplantation was associated with higher posttransplant disease and mortality.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e70003"},"PeriodicalIF":2.6000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12205293/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mycobacterium abscessus Complex Infections Among Lung Transplant Recipients: A Multicenter Retrospective Cohort Study in Canada.\",\"authors\":\"Roni Bitterman, Hafid Soualhine, Pierre-Marie Akochy, Charles Poirier, Pasquale Ferraro, Dima Kabbani, Alim Hirji, Gregory Tyrrell, Celine Bergeron, Robert D Levy, Alissa Wright, Victor Leung, Lianne G Singer, Cecilia Chaparro, Shaf Keshavjee, Melissa Richard-Greenblatt, Shahid Husain, Me-Linh Luong\",\"doi\":\"10.1111/tid.70003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Mycobacterium abscessus complex is known to cause life-threatening disease in lung transplantation (LT) recipients (LTRs). Therefore, many centers consider the presence of M. abscessus as a relative contraindication to LT.</p><p><strong>Methods: </strong>We conducted a multicenter retrospective cohort study including all 4 LT centers in Canada. All LTRs transplanted in 2006-2016 with at least one respiratory sample positive for M. abscessus prior or posttransplantation were included. Pulmonary disease was defined using the American Thoracic Society criteria. Minimal follow-up duration was 5 years after transplantation.</p><p><strong>Results: </strong>Among 2181 LTRs across Canada, 14 had M. abscessus disease after LT (incidence rate 1.1/1000 transplant-years) and 6 had pulmonary colonization (incidence rate 0.5/1000 transplant-years). Fifteen patients had M. abscessus cultured before LT. Among those with pretransplant M. abscessus, 53% (8/15) developed M. abscessus infection posttransplant (6 disease, 2 colonization). Posttransplant disease was less frequent among those with microbiologic eradication before transplant (0% vs. 85.7%, p = 0.001). LTRs with pretransplant M. abscessus had comparable survival to those without M. abscessus (log rank p = 0.37). Among patients with pretransplant infection, mortality was higher in those who did not achieve microbiological eradication before transplantation (57.1% vs. 0%, p = 0.03) and those who developed disease after transplantation (66.7% vs. 0%, p = 0.01).</p><p><strong>Conclusions: </strong>M. abscessus is an uncommon cause of infection among LTRs. Survival among those with pretransplant M. abscessus infection was similar to that observed in noninfected LTRs. However, lack of eradication before transplantation was associated with higher posttransplant disease and mortality.</p>\",\"PeriodicalId\":23318,\"journal\":{\"name\":\"Transplant Infectious Disease\",\"volume\":\" \",\"pages\":\"e70003\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12205293/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplant Infectious Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/tid.70003\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.70003","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:已知脓肿分枝杆菌复合体在肺移植(LT)受者(lts)中引起危及生命的疾病。因此,许多中心认为脓肿分枝杆菌的存在是肝移植的相对禁忌症。方法:我们进行了一项包括加拿大所有4个肝移植中心的多中心回顾性队列研究。所有2006-2016年移植且移植前或移植后至少有一个呼吸样本为脓肿分枝杆菌阳性的ltr纳入研究。肺部疾病的定义采用美国胸科学会的标准。移植后最短随访时间为5年。结果:在加拿大2181例ltr中,14例移植后发生脓肿分枝杆菌病(发病率1.1/1000移植年),6例发生肺定植(发病率0.5/1000移植年)。移植前有脓肿支原体培养的患者15例。移植前有脓肿支原体的患者中,53%(8/15)在移植后发生脓肿支原体感染(6例发病,2例定植)。移植前清除微生物的患者移植后疾病发生率较低(0% vs. 85.7%, p = 0.001)。移植前有脓肿分枝杆菌的ltr与没有脓肿分枝杆菌的ltr的生存率相当(log rank p = 0.37)。在移植前感染的患者中,移植前未实现微生物根除的患者死亡率更高(57.1%比0%,p = 0.03),移植后发生疾病的患者死亡率更高(66.7%比0%,p = 0.01)。结论:脓肿支原体是一种罕见的感染原因。移植前感染脓肿分枝杆菌的患者的生存率与未感染的ltr患者相似。然而,移植前缺乏根除与较高的移植后疾病和死亡率相关。
Mycobacterium abscessus Complex Infections Among Lung Transplant Recipients: A Multicenter Retrospective Cohort Study in Canada.
Background: Mycobacterium abscessus complex is known to cause life-threatening disease in lung transplantation (LT) recipients (LTRs). Therefore, many centers consider the presence of M. abscessus as a relative contraindication to LT.
Methods: We conducted a multicenter retrospective cohort study including all 4 LT centers in Canada. All LTRs transplanted in 2006-2016 with at least one respiratory sample positive for M. abscessus prior or posttransplantation were included. Pulmonary disease was defined using the American Thoracic Society criteria. Minimal follow-up duration was 5 years after transplantation.
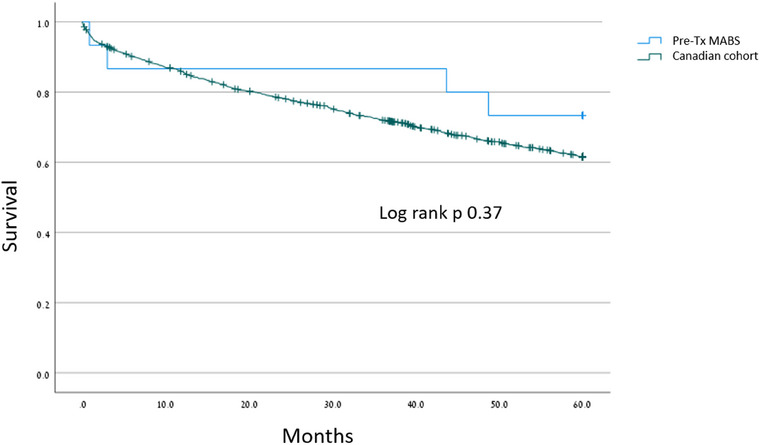
Results: Among 2181 LTRs across Canada, 14 had M. abscessus disease after LT (incidence rate 1.1/1000 transplant-years) and 6 had pulmonary colonization (incidence rate 0.5/1000 transplant-years). Fifteen patients had M. abscessus cultured before LT. Among those with pretransplant M. abscessus, 53% (8/15) developed M. abscessus infection posttransplant (6 disease, 2 colonization). Posttransplant disease was less frequent among those with microbiologic eradication before transplant (0% vs. 85.7%, p = 0.001). LTRs with pretransplant M. abscessus had comparable survival to those without M. abscessus (log rank p = 0.37). Among patients with pretransplant infection, mortality was higher in those who did not achieve microbiological eradication before transplantation (57.1% vs. 0%, p = 0.03) and those who developed disease after transplantation (66.7% vs. 0%, p = 0.01).
Conclusions: M. abscessus is an uncommon cause of infection among LTRs. Survival among those with pretransplant M. abscessus infection was similar to that observed in noninfected LTRs. However, lack of eradication before transplantation was associated with higher posttransplant disease and mortality.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



