Sih-Yao Chen, Jheng-Yan Wu, Kuang-Ming Liao, Yu-Min Lin
{"title":"GLP-1 RA加SGLT2i对ASCVD和心力衰竭患者预后的益处:一项队列研究","authors":"Sih-Yao Chen, Jheng-Yan Wu, Kuang-Ming Liao, Yu-Min Lin","doi":"10.1093/ehjcvp/pvaf014","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Managing patients with atherosclerotic cardiovascular disease (ASCVD) and heart failure (HF) is challenging. While sodium-glucose cotransporter 2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA) show cardiovascular benefits, the impact of combining these agents is unclear. This study evaluated whether adding GLP-1 RA to SGLT2i provides additional benefits in patients with both ASCVD and HF.</p><p><strong>Methods and results: </strong>This retrospective observational study utilized the TriNetX database to analyse patients with ASCVD and HF who initiated GLP-1 RA with SGLT2i or SGLT2i alone from 1 August 2016 to 30 September 2024. A total of 2 797 317 patients were identified, with 96 051 patients meeting inclusion criteria. After propensity score matching, 5272 patients in each group were analysed. Primary outcomes included mortality or hospitalization within 1 year; secondary outcomes examined mortality, hospitalization, and heart failure exacerbation (HFE). Patients receiving GLP-1RA and SGLT2i therapies had significantly lower risk of mortality or hospitalization [hazard ratio (HR) 0.78; 95% confidence interval (CI) 0.74-0.83], mortality (HR 0.72; 95% CI 0.62-0.84), hospitalization (HR 0.78; 95% CI 0.73-0.83), and HFE (HR 0.77; 95% CI 0.72-0.83) vs. SGLT2i alone. Subgroup analyses showed consistent benefits in patients with HFpEF, HFrEF, patients with diabetes, obesity, chronic kidney disease, or those using semaglutide or dulaglutide, while liraglutide use showed a neutral effect. Drug-related side effects were monitored as safety outcomes, which showed no significant differences between groups.</p><p><strong>Conclusions: </strong>In ASCVD and HF patients, adding GLP-1 RA to SGLT2i reduces 1-year mortality and hospitalization, warranting further investigation in diverse settings.</p>","PeriodicalId":11982,"journal":{"name":"European Heart Journal - Cardiovascular Pharmacotherapy","volume":" ","pages":"324-333"},"PeriodicalIF":6.1000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12231126/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic benefit of glucagon-like peptide-1 receptor agonists addition to sodium-glucose cotransporter 2 inhibitors in patients with atherosclerotic cardiovascular disease and heart failure: a cohort study.\",\"authors\":\"Sih-Yao Chen, Jheng-Yan Wu, Kuang-Ming Liao, Yu-Min Lin\",\"doi\":\"10.1093/ehjcvp/pvaf014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Managing patients with atherosclerotic cardiovascular disease (ASCVD) and heart failure (HF) is challenging. While sodium-glucose cotransporter 2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA) show cardiovascular benefits, the impact of combining these agents is unclear. This study evaluated whether adding GLP-1 RA to SGLT2i provides additional benefits in patients with both ASCVD and HF.</p><p><strong>Methods and results: </strong>This retrospective observational study utilized the TriNetX database to analyse patients with ASCVD and HF who initiated GLP-1 RA with SGLT2i or SGLT2i alone from 1 August 2016 to 30 September 2024. A total of 2 797 317 patients were identified, with 96 051 patients meeting inclusion criteria. After propensity score matching, 5272 patients in each group were analysed. Primary outcomes included mortality or hospitalization within 1 year; secondary outcomes examined mortality, hospitalization, and heart failure exacerbation (HFE). Patients receiving GLP-1RA and SGLT2i therapies had significantly lower risk of mortality or hospitalization [hazard ratio (HR) 0.78; 95% confidence interval (CI) 0.74-0.83], mortality (HR 0.72; 95% CI 0.62-0.84), hospitalization (HR 0.78; 95% CI 0.73-0.83), and HFE (HR 0.77; 95% CI 0.72-0.83) vs. SGLT2i alone. Subgroup analyses showed consistent benefits in patients with HFpEF, HFrEF, patients with diabetes, obesity, chronic kidney disease, or those using semaglutide or dulaglutide, while liraglutide use showed a neutral effect. Drug-related side effects were monitored as safety outcomes, which showed no significant differences between groups.</p><p><strong>Conclusions: </strong>In ASCVD and HF patients, adding GLP-1 RA to SGLT2i reduces 1-year mortality and hospitalization, warranting further investigation in diverse settings.</p>\",\"PeriodicalId\":11982,\"journal\":{\"name\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"volume\":\" \",\"pages\":\"324-333\"},\"PeriodicalIF\":6.1000,\"publicationDate\":\"2025-07-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12231126/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjcvp/pvaf014\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvaf014","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
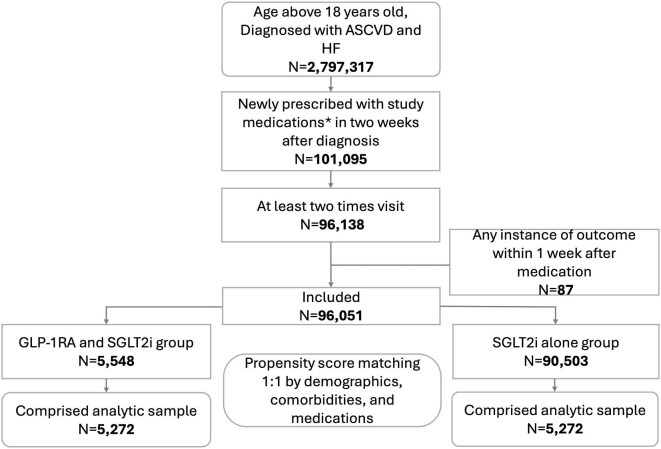
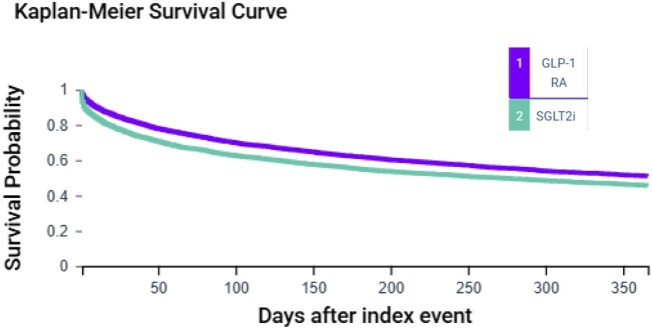
目的:管理动脉粥样硬化性心血管疾病(ASCVD)和心力衰竭(HF)患者具有挑战性。虽然钠-葡萄糖共转运蛋白2抑制剂(SGLT2i)和胰高血糖素样肽-1受体激动剂(GLP-1 RA)显示心血管益处,但联合使用这些药物的影响尚不清楚。本研究评估了在SGLT2i基础上添加GLP-1 RA是否能为ASCVD和HF患者提供额外的益处。方法和结果:这项回顾性观察性研究利用TriNetX数据库分析了2016年8月1日至2024年9月30日期间,联合SGLT2i或单独使用SGLT2i启动GLP-1 RA的ASCVD和HF患者。共纳入2 797 317例患者,其中96 051例符合纳入标准。经倾向评分匹配(PSM),对两组5 272例患者进行分析。主要结局包括一年内的死亡率或住院率;次要结局检查死亡率、住院率和心力衰竭加重(HFE)。接受GLP-1RA和SGLT2i治疗的患者死亡或住院风险显著降低(HR 0.78;95% CI 0.74-0.83),死亡率(HR 0.72;95% CI 0.62-0.84),住院率(HR 0.78;95% CI 0.73-0.83)和HFE (HR 0.77;95% CI 0.72-0.83)与单纯SGLT2i相比。亚组分析显示HFpEF、HFrEF患者、糖尿病、肥胖、慢性肾脏疾病患者或使用semaglutide或dulaglutide的患者均有一致的益处,而利拉鲁肽的使用显示中性效果。药物相关副作用作为安全结果进行监测,各组间无显著差异。结论:在ASCVD和HF患者中,将GLP-1 RA加入SGLT2i可降低一年死亡率和住院率,值得在不同情况下进一步研究。
Prognostic benefit of glucagon-like peptide-1 receptor agonists addition to sodium-glucose cotransporter 2 inhibitors in patients with atherosclerotic cardiovascular disease and heart failure: a cohort study.
Aims: Managing patients with atherosclerotic cardiovascular disease (ASCVD) and heart failure (HF) is challenging. While sodium-glucose cotransporter 2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA) show cardiovascular benefits, the impact of combining these agents is unclear. This study evaluated whether adding GLP-1 RA to SGLT2i provides additional benefits in patients with both ASCVD and HF.
Methods and results: This retrospective observational study utilized the TriNetX database to analyse patients with ASCVD and HF who initiated GLP-1 RA with SGLT2i or SGLT2i alone from 1 August 2016 to 30 September 2024. A total of 2 797 317 patients were identified, with 96 051 patients meeting inclusion criteria. After propensity score matching, 5272 patients in each group were analysed. Primary outcomes included mortality or hospitalization within 1 year; secondary outcomes examined mortality, hospitalization, and heart failure exacerbation (HFE). Patients receiving GLP-1RA and SGLT2i therapies had significantly lower risk of mortality or hospitalization [hazard ratio (HR) 0.78; 95% confidence interval (CI) 0.74-0.83], mortality (HR 0.72; 95% CI 0.62-0.84), hospitalization (HR 0.78; 95% CI 0.73-0.83), and HFE (HR 0.77; 95% CI 0.72-0.83) vs. SGLT2i alone. Subgroup analyses showed consistent benefits in patients with HFpEF, HFrEF, patients with diabetes, obesity, chronic kidney disease, or those using semaglutide or dulaglutide, while liraglutide use showed a neutral effect. Drug-related side effects were monitored as safety outcomes, which showed no significant differences between groups.
Conclusions: In ASCVD and HF patients, adding GLP-1 RA to SGLT2i reduces 1-year mortality and hospitalization, warranting further investigation in diverse settings.
期刊介绍:
The European Heart Journal - Cardiovascular Pharmacotherapy (EHJ-CVP) is an international, peer-reviewed journal published in English, specifically dedicated to clinical cardiovascular pharmacology. EHJ-CVP publishes original articles focusing on clinical research involving both new and established drugs and methods, along with meta-analyses and topical reviews. The journal's primary aim is to enhance the pharmacological treatment of patients with cardiovascular disease by interpreting and integrating new scientific developments in this field.
While the emphasis is on clinical topics, EHJ-CVP also considers basic research articles from fields such as physiology and molecular biology that contribute to the understanding of cardiovascular drug therapy. These may include articles related to new drug development and evaluation, the physiological and pharmacological basis of drug action, metabolism, drug interactions, and side effects.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


