S Ge, Z Feng, L Lin, R Li, Y Zhang, L Song, A Wang, Y Lan, Y Li, Z Huang, C Cai, X Wang, Q Ruan, H Yu, M Tang, H Yi, Y Chen, F Sun, Y Li, W Zhang
{"title":"耐利福平结核病诊断和治疗延误的患者途径分析。","authors":"S Ge, Z Feng, L Lin, R Li, Y Zhang, L Song, A Wang, Y Lan, Y Li, Z Huang, C Cai, X Wang, Q Ruan, H Yu, M Tang, H Yi, Y Chen, F Sun, Y Li, W Zhang","doi":"10.5588/ijtldopen.24.0469","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Barriers to the diagnosis and treatment of rifampicin-resistant TB (RR-TB) have not been fully elucidated. This study aimed to map the diagnostic and treatment delays among patients with RR-TB in China and investigate related factors.</p><p><strong>Methods: </strong>Between June and July 2023, the diagnostic and treatment pathways of patients with RR-TB were obtained through interviews at eight hospitals across China. Information on the TB service of hospitals was collected via telephone.</p><p><strong>Results: </strong>Ninety-eight patients were included. On average, each patient required 4.6 visits to start RR-TB treatment. The median delay from illness onset to RR-TB treatment was 238.0 days (IQR 85.8-469.2), primarily driven by the delay between TB diagnosis and identifying rifampicin (RIF) resistance (median: 43.5 days, IQR 3.0-160.5). Referral to appropriate hospitals (adjusted hazard ratio [aHR] 2.32; 95% CI 1.37-3.92) or considering drug susceptibility testing (DST) when initiating treatment (aHR 2.56, 95% CI 1.39-4.72) significantly reduced delay between TB diagnosis and identifying RIF resistance, while stigma regarding TB (aHR 0.61, 95% CI 0.38-0.98) was an independent risk factor.</p><p><strong>Conclusions: </strong>Patients with RR-TB experienced substantial delays in identifying RIF resistance. Referring patients to hospitals with molecular DST capabilities and awareness may reduce these delays.</p>","PeriodicalId":519984,"journal":{"name":"IJTLD open","volume":"2 2","pages":"90-95"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11827674/pdf/","citationCount":"0","resultStr":"{\"title\":\"Patient pathway analysis of rifampicin-resistant TB diagnostic and treatment delays.\",\"authors\":\"S Ge, Z Feng, L Lin, R Li, Y Zhang, L Song, A Wang, Y Lan, Y Li, Z Huang, C Cai, X Wang, Q Ruan, H Yu, M Tang, H Yi, Y Chen, F Sun, Y Li, W Zhang\",\"doi\":\"10.5588/ijtldopen.24.0469\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Barriers to the diagnosis and treatment of rifampicin-resistant TB (RR-TB) have not been fully elucidated. This study aimed to map the diagnostic and treatment delays among patients with RR-TB in China and investigate related factors.</p><p><strong>Methods: </strong>Between June and July 2023, the diagnostic and treatment pathways of patients with RR-TB were obtained through interviews at eight hospitals across China. Information on the TB service of hospitals was collected via telephone.</p><p><strong>Results: </strong>Ninety-eight patients were included. On average, each patient required 4.6 visits to start RR-TB treatment. The median delay from illness onset to RR-TB treatment was 238.0 days (IQR 85.8-469.2), primarily driven by the delay between TB diagnosis and identifying rifampicin (RIF) resistance (median: 43.5 days, IQR 3.0-160.5). Referral to appropriate hospitals (adjusted hazard ratio [aHR] 2.32; 95% CI 1.37-3.92) or considering drug susceptibility testing (DST) when initiating treatment (aHR 2.56, 95% CI 1.39-4.72) significantly reduced delay between TB diagnosis and identifying RIF resistance, while stigma regarding TB (aHR 0.61, 95% CI 0.38-0.98) was an independent risk factor.</p><p><strong>Conclusions: </strong>Patients with RR-TB experienced substantial delays in identifying RIF resistance. Referring patients to hospitals with molecular DST capabilities and awareness may reduce these delays.</p>\",\"PeriodicalId\":519984,\"journal\":{\"name\":\"IJTLD open\",\"volume\":\"2 2\",\"pages\":\"90-95\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11827674/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"IJTLD open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5588/ijtldopen.24.0469\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJTLD open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5588/ijtldopen.24.0469","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:诊断和治疗利福平耐药结核病(RR-TB)的障碍尚未完全阐明。本研究旨在了解中国RR-TB患者的诊断和治疗延误情况,并探讨相关因素。方法:于2023年6月至7月,通过对全国8家医院的访谈,获取RR-TB患者的诊断和治疗途径。通过电话收集了有关医院结核病服务的信息。结果:纳入98例患者。平均而言,每位患者需要4.6次就诊才能开始接受耐药结核病治疗。从发病到接受RR-TB治疗的中位延迟为238.0天(IQR为85.8-469.2),主要是由于结核病诊断到发现利福平(RIF)耐药性之间的延迟(中位:43.5天,IQR为3.0-160.5)。转诊到合适的医院(调整风险比[aHR] 2.32;95% CI 1.37-3.92)或在开始治疗时考虑药敏试验(DST) (aHR 2.56, 95% CI 1.39-4.72)可显著减少结核病诊断和确定RIF耐药之间的延迟,而结核病的耻辱(aHR 0.61, 95% CI 0.38-0.98)是一个独立的危险因素。结论:RR-TB患者在识别RIF耐药性方面经历了严重的延迟。将患者转到具有分子DST能力和意识的医院可能会减少这些延误。
Patient pathway analysis of rifampicin-resistant TB diagnostic and treatment delays.
Background: Barriers to the diagnosis and treatment of rifampicin-resistant TB (RR-TB) have not been fully elucidated. This study aimed to map the diagnostic and treatment delays among patients with RR-TB in China and investigate related factors.
Methods: Between June and July 2023, the diagnostic and treatment pathways of patients with RR-TB were obtained through interviews at eight hospitals across China. Information on the TB service of hospitals was collected via telephone.
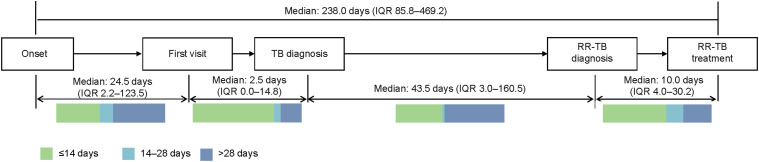
Results: Ninety-eight patients were included. On average, each patient required 4.6 visits to start RR-TB treatment. The median delay from illness onset to RR-TB treatment was 238.0 days (IQR 85.8-469.2), primarily driven by the delay between TB diagnosis and identifying rifampicin (RIF) resistance (median: 43.5 days, IQR 3.0-160.5). Referral to appropriate hospitals (adjusted hazard ratio [aHR] 2.32; 95% CI 1.37-3.92) or considering drug susceptibility testing (DST) when initiating treatment (aHR 2.56, 95% CI 1.39-4.72) significantly reduced delay between TB diagnosis and identifying RIF resistance, while stigma regarding TB (aHR 0.61, 95% CI 0.38-0.98) was an independent risk factor.
Conclusions: Patients with RR-TB experienced substantial delays in identifying RIF resistance. Referring patients to hospitals with molecular DST capabilities and awareness may reduce these delays.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


