{"title":"日本9-10岁儿童普遍筛查与家族性高胆固醇血症亲属反级联筛查相结合的成本-效果分析","authors":"Keiji Matsunaga, Mariko Harada-Shiba, Shizuya Yamashita, Hayato Tada, Akihito Uda, Katsuya Mori, Mizuki Yoshimura, Sachie Inoue, Isao Kamae, Shinji Yokoyama, Tetsuo Minamino","doi":"10.5551/jat.65181","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Screening for familial hypercholesterolemia (FH) is important for reducing the incidence of cardiovascular diseases (CVDs). Cost-effectiveness was evaluated using the Kagawa FH screening model, which is a combination of universal screening (US) in the universal health examination for children 9-10 years old conducted in Kagawa Prefecture, and reverse cascade screening (RCS) of the probands' relatives.</p><p><strong>Methods: </strong>A lifetime simulation was conducted using mathematical models (decision tree and Markov model) to determine the cost-effectiveness of introducing a series of FH screenings (US in children + RCS in adult relatives). Only screening-related costs and direct medical costs were included, using quality-adjusted life years (QALYs) as an outcome. The costs of statins were estimated using the public health insurance claims database DeSC Healthcare, Inc. The risk of each CVD event was estimated using the same claims data and adjusted for age. We hypothesized that standard statin treatment decreases CVD risk by reducing plasma low-density lipoprotein cholesterol levels.</p><p><strong>Results: </strong>A series of FH screenings (US in children + RCS in adult relatives) was cost-effective compared to no screening, with an incremental cost-effectiveness ratio (ICER) of approximately JPY 150,000 (USD 1,042)/QALY, which was below the willingness-to-pay threshold of JPY 5,000,000 (USD 34,722)/QALY for medical technology in Japan (USD 1 = JPY 144). The ICER for the US without RCS was also acceptable at approximately JPY 2,720,000 (USD 18,889)/QALY.</p><p><strong>Conclusion: </strong>The cost-effectiveness analysis revealed that a series of FH screenings (US in children + RCS in adult relatives) based on the Kagawa model was cost-effective.</p>","PeriodicalId":15128,"journal":{"name":"Journal of atherosclerosis and thrombosis","volume":" ","pages":"962-981"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12328689/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Cost-Effectiveness Analysis for the Combination of Universal Screening at 9-10 Years Old and Reverse Cascade Screening of Relatives for Familial Hypercholesterolemia in Japan.\",\"authors\":\"Keiji Matsunaga, Mariko Harada-Shiba, Shizuya Yamashita, Hayato Tada, Akihito Uda, Katsuya Mori, Mizuki Yoshimura, Sachie Inoue, Isao Kamae, Shinji Yokoyama, Tetsuo Minamino\",\"doi\":\"10.5551/jat.65181\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>Screening for familial hypercholesterolemia (FH) is important for reducing the incidence of cardiovascular diseases (CVDs). Cost-effectiveness was evaluated using the Kagawa FH screening model, which is a combination of universal screening (US) in the universal health examination for children 9-10 years old conducted in Kagawa Prefecture, and reverse cascade screening (RCS) of the probands' relatives.</p><p><strong>Methods: </strong>A lifetime simulation was conducted using mathematical models (decision tree and Markov model) to determine the cost-effectiveness of introducing a series of FH screenings (US in children + RCS in adult relatives). Only screening-related costs and direct medical costs were included, using quality-adjusted life years (QALYs) as an outcome. The costs of statins were estimated using the public health insurance claims database DeSC Healthcare, Inc. The risk of each CVD event was estimated using the same claims data and adjusted for age. We hypothesized that standard statin treatment decreases CVD risk by reducing plasma low-density lipoprotein cholesterol levels.</p><p><strong>Results: </strong>A series of FH screenings (US in children + RCS in adult relatives) was cost-effective compared to no screening, with an incremental cost-effectiveness ratio (ICER) of approximately JPY 150,000 (USD 1,042)/QALY, which was below the willingness-to-pay threshold of JPY 5,000,000 (USD 34,722)/QALY for medical technology in Japan (USD 1 = JPY 144). The ICER for the US without RCS was also acceptable at approximately JPY 2,720,000 (USD 18,889)/QALY.</p><p><strong>Conclusion: </strong>The cost-effectiveness analysis revealed that a series of FH screenings (US in children + RCS in adult relatives) based on the Kagawa model was cost-effective.</p>\",\"PeriodicalId\":15128,\"journal\":{\"name\":\"Journal of atherosclerosis and thrombosis\",\"volume\":\" \",\"pages\":\"962-981\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12328689/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of atherosclerosis and thrombosis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5551/jat.65181\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of atherosclerosis and thrombosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5551/jat.65181","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
A Cost-Effectiveness Analysis for the Combination of Universal Screening at 9-10 Years Old and Reverse Cascade Screening of Relatives for Familial Hypercholesterolemia in Japan.
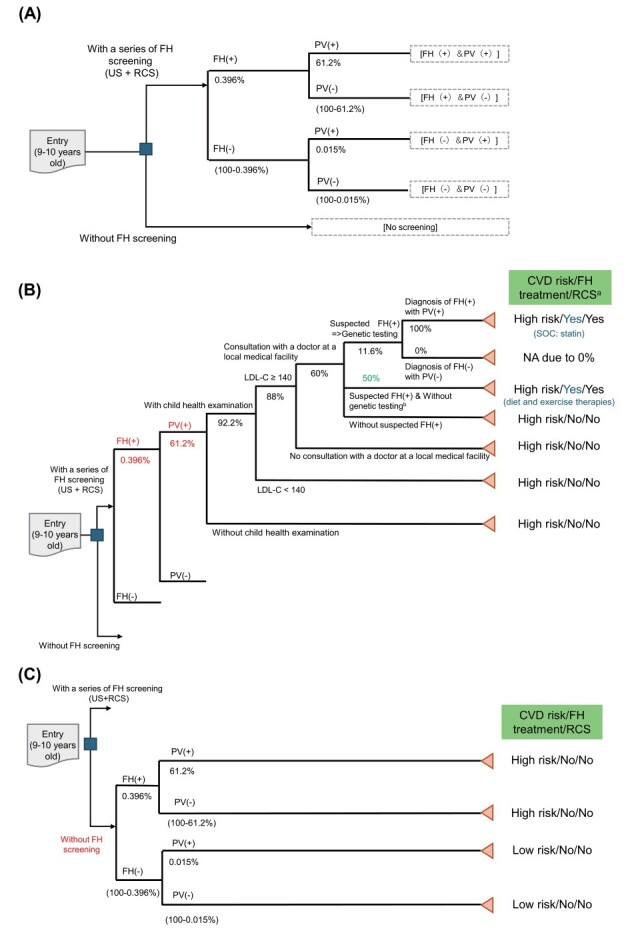
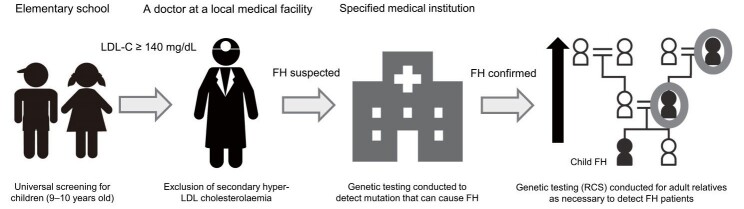
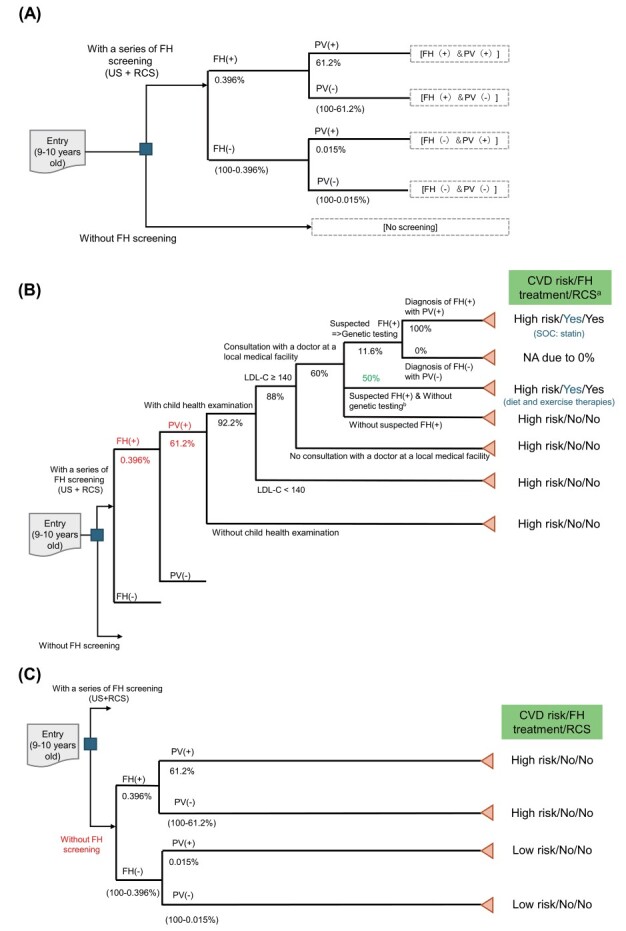
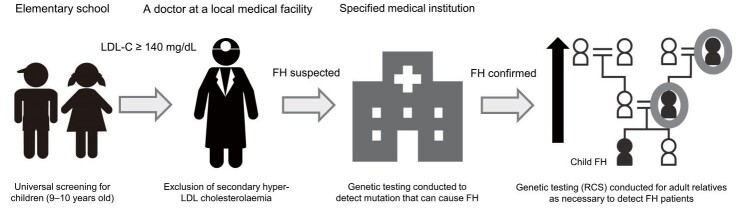
Aim: Screening for familial hypercholesterolemia (FH) is important for reducing the incidence of cardiovascular diseases (CVDs). Cost-effectiveness was evaluated using the Kagawa FH screening model, which is a combination of universal screening (US) in the universal health examination for children 9-10 years old conducted in Kagawa Prefecture, and reverse cascade screening (RCS) of the probands' relatives.
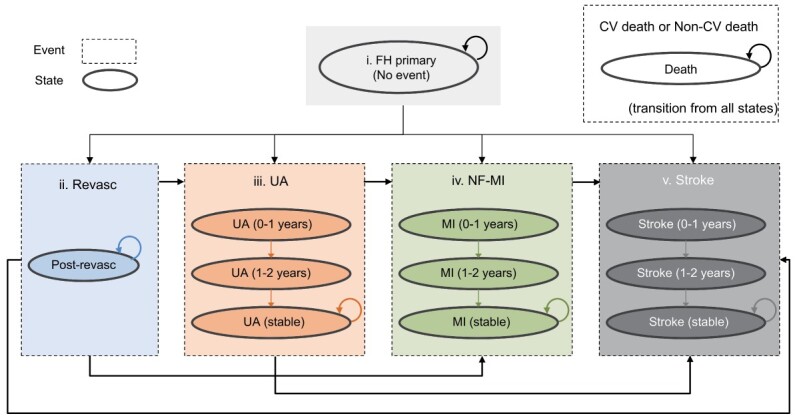
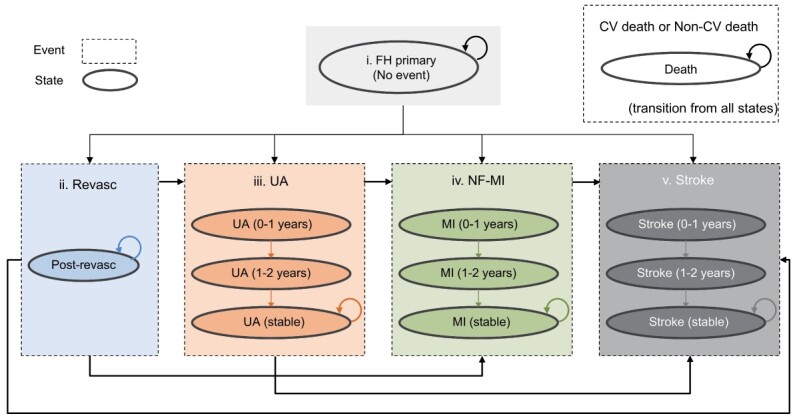
Methods: A lifetime simulation was conducted using mathematical models (decision tree and Markov model) to determine the cost-effectiveness of introducing a series of FH screenings (US in children + RCS in adult relatives). Only screening-related costs and direct medical costs were included, using quality-adjusted life years (QALYs) as an outcome. The costs of statins were estimated using the public health insurance claims database DeSC Healthcare, Inc. The risk of each CVD event was estimated using the same claims data and adjusted for age. We hypothesized that standard statin treatment decreases CVD risk by reducing plasma low-density lipoprotein cholesterol levels.
Results: A series of FH screenings (US in children + RCS in adult relatives) was cost-effective compared to no screening, with an incremental cost-effectiveness ratio (ICER) of approximately JPY 150,000 (USD 1,042)/QALY, which was below the willingness-to-pay threshold of JPY 5,000,000 (USD 34,722)/QALY for medical technology in Japan (USD 1 = JPY 144). The ICER for the US without RCS was also acceptable at approximately JPY 2,720,000 (USD 18,889)/QALY.
Conclusion: The cost-effectiveness analysis revealed that a series of FH screenings (US in children + RCS in adult relatives) based on the Kagawa model was cost-effective.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


