Mohsen Mohammadi, Bima J Hasjim, Salva N Balbale, Praneet Polineni, Alexander A Huang, Mitchell Paukner, Therese Banea, Oriana Dentici, Dominic J Vitello, Joy E Obayemi, Andrés Duarte-Rojo, Satish N Nadig, Lisa B VanWagner, Lihui Zhao, Sanjay Mehrotra, Daniela P Ladner
{"title":"美国肝硬化患者的疾病发展轨迹和竞争风险","authors":"Mohsen Mohammadi, Bima J Hasjim, Salva N Balbale, Praneet Polineni, Alexander A Huang, Mitchell Paukner, Therese Banea, Oriana Dentici, Dominic J Vitello, Joy E Obayemi, Andrés Duarte-Rojo, Satish N Nadig, Lisa B VanWagner, Lihui Zhao, Sanjay Mehrotra, Daniela P Ladner","doi":"10.1371/journal.pone.0313152","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cirrhosis is a dynamic disease process leading to liver-related death, which has increased by over 65% over the last decade. Unpredictable hepatic decompensation complications are a major source of morbidity and mortality. Thus, accurately characterizing disease progression through discrete stages of cirrhosis is critical towards implementing timely intervention and liver transplant (LT) waitlisting.</p><p><strong>Methods: </strong>A retrospective, longitudinal, population-cohort study of adult patients with cirrhosis from a US metropolitan area (2006-2012) was conducted. Clinical diagnoses were defined by ICD-9 and CPT codes. Cirrhosis stages were defined as: compensated without portal hypertension (Stage 1), compensated with portal hypertension (Stage 2), variceal bleeding (Stage 3), hepatic encephalopathy (Stage 4a), ascites (Stage 4b), and ≥2 different decompensating complications (Stage 5). Multivariate Fine-Gray competing risk survival analysis adjusted for clinicodemographic covariates.</p><p><strong>Results: </strong>Among 12,196 patients with cirrhosis, the mean (±SD) age was 56.8 (±11.7) years with a follow-up time of 2.35 (±1.81) years. A novel 5-stage disease progression framework was used. The 1-year mortality rates for each stage were 7.3% for Stage 1, 5.4% for Stage 2, 11.4% for Stage 3, 10.0% for Stage 4a, 20.2% for Stage 4b, and 43.8% for Stage 5. Compared to those in Stage 1, Stage 3 (sHR:1.83, 95% CI:1.36-2.48, P<0.001), Stage 4b (sHR:1.45, 95% CI:1.23-1.70, P<0.001), and Stage 5 (sHR:1.95, 95% CI:1.71-2.23, P<0.001) patients had higher risks of mortality. Additional disease progression rates were identified.</p><p><strong>Conclusion: </strong>Even among patients with compensated cirrhosis, the 1-year mortality rate was as high as 7.3% and subsequently increases with each decompensation complication. This one-year mortality rate is higher than 5-years mortality rate reported in previously known non-US studies. The highest associated risk of death was observed among patients with ≥2 different decompensating complications (95.2%), variceal bleeding (83.2%) and ascites (44.9%). Overall, patients in advanced stages of cirrhosis were more likely to die than they were to receive a LT, suggesting that patients should be referred and waitlisted for LT earlier in the disease process.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 2","pages":"e0313152"},"PeriodicalIF":2.6000,"publicationDate":"2025-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11828360/pdf/","citationCount":"0","resultStr":"{\"title\":\"Disease trajectory and competing risks of patients with cirrhosis in the US.\",\"authors\":\"Mohsen Mohammadi, Bima J Hasjim, Salva N Balbale, Praneet Polineni, Alexander A Huang, Mitchell Paukner, Therese Banea, Oriana Dentici, Dominic J Vitello, Joy E Obayemi, Andrés Duarte-Rojo, Satish N Nadig, Lisa B VanWagner, Lihui Zhao, Sanjay Mehrotra, Daniela P Ladner\",\"doi\":\"10.1371/journal.pone.0313152\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cirrhosis is a dynamic disease process leading to liver-related death, which has increased by over 65% over the last decade. Unpredictable hepatic decompensation complications are a major source of morbidity and mortality. Thus, accurately characterizing disease progression through discrete stages of cirrhosis is critical towards implementing timely intervention and liver transplant (LT) waitlisting.</p><p><strong>Methods: </strong>A retrospective, longitudinal, population-cohort study of adult patients with cirrhosis from a US metropolitan area (2006-2012) was conducted. Clinical diagnoses were defined by ICD-9 and CPT codes. Cirrhosis stages were defined as: compensated without portal hypertension (Stage 1), compensated with portal hypertension (Stage 2), variceal bleeding (Stage 3), hepatic encephalopathy (Stage 4a), ascites (Stage 4b), and ≥2 different decompensating complications (Stage 5). Multivariate Fine-Gray competing risk survival analysis adjusted for clinicodemographic covariates.</p><p><strong>Results: </strong>Among 12,196 patients with cirrhosis, the mean (±SD) age was 56.8 (±11.7) years with a follow-up time of 2.35 (±1.81) years. A novel 5-stage disease progression framework was used. The 1-year mortality rates for each stage were 7.3% for Stage 1, 5.4% for Stage 2, 11.4% for Stage 3, 10.0% for Stage 4a, 20.2% for Stage 4b, and 43.8% for Stage 5. Compared to those in Stage 1, Stage 3 (sHR:1.83, 95% CI:1.36-2.48, P<0.001), Stage 4b (sHR:1.45, 95% CI:1.23-1.70, P<0.001), and Stage 5 (sHR:1.95, 95% CI:1.71-2.23, P<0.001) patients had higher risks of mortality. Additional disease progression rates were identified.</p><p><strong>Conclusion: </strong>Even among patients with compensated cirrhosis, the 1-year mortality rate was as high as 7.3% and subsequently increases with each decompensation complication. This one-year mortality rate is higher than 5-years mortality rate reported in previously known non-US studies. The highest associated risk of death was observed among patients with ≥2 different decompensating complications (95.2%), variceal bleeding (83.2%) and ascites (44.9%). Overall, patients in advanced stages of cirrhosis were more likely to die than they were to receive a LT, suggesting that patients should be referred and waitlisted for LT earlier in the disease process.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 2\",\"pages\":\"e0313152\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-02-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11828360/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0313152\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0313152","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Disease trajectory and competing risks of patients with cirrhosis in the US.
Background: Cirrhosis is a dynamic disease process leading to liver-related death, which has increased by over 65% over the last decade. Unpredictable hepatic decompensation complications are a major source of morbidity and mortality. Thus, accurately characterizing disease progression through discrete stages of cirrhosis is critical towards implementing timely intervention and liver transplant (LT) waitlisting.
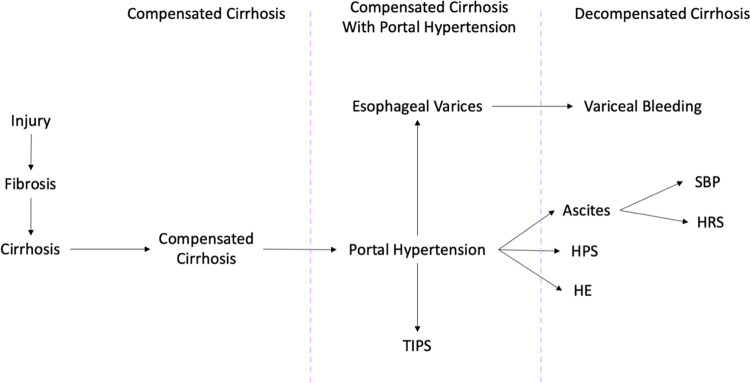
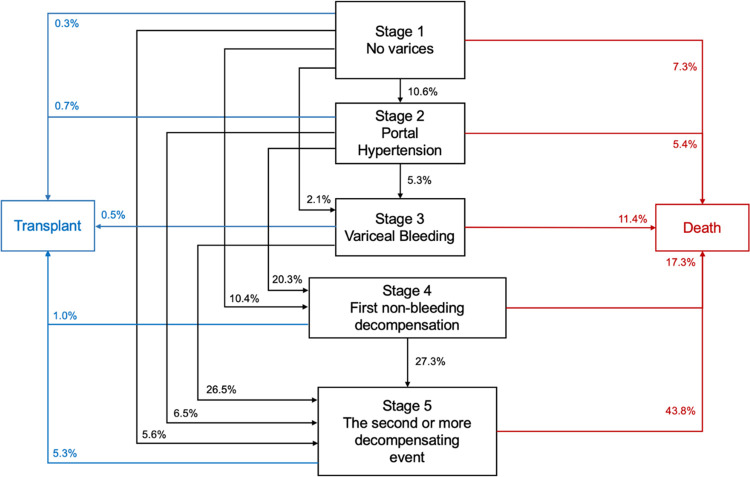
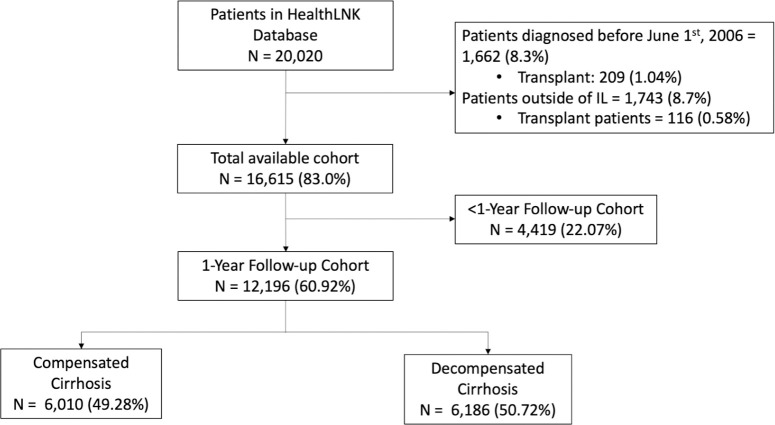
Methods: A retrospective, longitudinal, population-cohort study of adult patients with cirrhosis from a US metropolitan area (2006-2012) was conducted. Clinical diagnoses were defined by ICD-9 and CPT codes. Cirrhosis stages were defined as: compensated without portal hypertension (Stage 1), compensated with portal hypertension (Stage 2), variceal bleeding (Stage 3), hepatic encephalopathy (Stage 4a), ascites (Stage 4b), and ≥2 different decompensating complications (Stage 5). Multivariate Fine-Gray competing risk survival analysis adjusted for clinicodemographic covariates.
Results: Among 12,196 patients with cirrhosis, the mean (±SD) age was 56.8 (±11.7) years with a follow-up time of 2.35 (±1.81) years. A novel 5-stage disease progression framework was used. The 1-year mortality rates for each stage were 7.3% for Stage 1, 5.4% for Stage 2, 11.4% for Stage 3, 10.0% for Stage 4a, 20.2% for Stage 4b, and 43.8% for Stage 5. Compared to those in Stage 1, Stage 3 (sHR:1.83, 95% CI:1.36-2.48, P<0.001), Stage 4b (sHR:1.45, 95% CI:1.23-1.70, P<0.001), and Stage 5 (sHR:1.95, 95% CI:1.71-2.23, P<0.001) patients had higher risks of mortality. Additional disease progression rates were identified.
Conclusion: Even among patients with compensated cirrhosis, the 1-year mortality rate was as high as 7.3% and subsequently increases with each decompensation complication. This one-year mortality rate is higher than 5-years mortality rate reported in previously known non-US studies. The highest associated risk of death was observed among patients with ≥2 different decompensating complications (95.2%), variceal bleeding (83.2%) and ascites (44.9%). Overall, patients in advanced stages of cirrhosis were more likely to die than they were to receive a LT, suggesting that patients should be referred and waitlisted for LT earlier in the disease process.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


