Andrea Sauer, Klaus Stahl, Benjamin Seeliger, Pedro David Wendel-Garcia, Felix Lehmann, Julius J Schmidt, Bernhard M W Schmidt, Tobias Welte, Konrad Peukert, Lennart Wild, Christian Putensen, Sascha David, Christian Bode
{"title":"治疗性血浆置换对感染性休克炎症反应的影响:exchange -1试验的二次分析","authors":"Andrea Sauer, Klaus Stahl, Benjamin Seeliger, Pedro David Wendel-Garcia, Felix Lehmann, Julius J Schmidt, Bernhard M W Schmidt, Tobias Welte, Konrad Peukert, Lennart Wild, Christian Putensen, Sascha David, Christian Bode","doi":"10.1186/s40635-025-00725-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis and septic shock, defined by a profound immune dysregulation, are among the leading causes of death in the intensive care unit (ICU). Despite advances in understanding the underlying pathophysiology, evidence for specific immunomodulatory treatment does not exist to date. Therapeutic plasma exchange (TPE) represents an adjunctive treatment approach to rebalance immune homeostasis. In the EXCHANGE-1 trial, we recently demonstrated a rapid hemodynamic improvement, possibly caused by the removal of harmful mediators and the replacement of protective plasma proteins. The aim of this secondary analysis is to further characterize the underlying immunomodulatory effects and to identify biomarkers that may predict treatment response.</p><p><strong>Methods: </strong>This secondary analysis included patients in early septic shock (< 24 h duration) and a norepinephrine (NE) dose of ≥ 0.4 μg/kg/min. Patients were randomized 1:1 to receive standard of care (SOC) or SOC + one single TPE and plasma samples were collected before and after TPE. Within-group and between group effects of circulating levels of acute-phase proteins [CRP and Pentraxin3 (PTX3)], inflammatory mediators (IL-4, IL-6, IL-8, IL-10, TNF-α, IL-2Rα/CD25) and damage-associated molecular pattern (DAMP) [cell-free DNA (cfDNA)] were analyzed via paired t test or Wilcoxon signed-rank test and a mixed-effects model. Multivariate mixed-effects modeling of NE and lactate reduction was performed to investigate if cfDNA could be associated with treatment response to TPE.</p><p><strong>Results: </strong>TPE led to a significant reduction in circulating acute-phase protein levels (CRP p = 0.00976, PTX3 p = 0.0001). Pro-inflammatory cytokines, such as circulating TNF-α-, IL-6- und IL-8-levels, were significantly reduced in both groups with no significant difference between treatment groups except for IL-2Rα/CD25 (p ≤ 0.0001). In a multivariate mixed-effects model, rising cfDNA levels over the first 6 h indicated refractoriness to SOC treatment regarding NE (p = 0.004) and lactate (p = 0.001), whereas those receiving TPE demonstrated sustained reductions in both parameters.</p><p><strong>Conclusions: </strong>In this secondary analysis of the EXCHANGE-1 trial adjunctive TPE is associated with the reduction of acute-phase proteins and IL-2Rα/CD25, however not with the reduction of pro-inflammatory cytokines. This phenomenon could contribute to the observed enhancement in hemodynamics among patients with septic shock. Furthermore, TPE may be particularly beneficial for patients with septic shock who exhibit rising levels of cfDNA.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"18"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11828778/pdf/","citationCount":"0","resultStr":"{\"title\":\"The effect of therapeutic plasma exchange on the inflammatory response in septic shock: a secondary analysis of the EXCHANGE-1 trial.\",\"authors\":\"Andrea Sauer, Klaus Stahl, Benjamin Seeliger, Pedro David Wendel-Garcia, Felix Lehmann, Julius J Schmidt, Bernhard M W Schmidt, Tobias Welte, Konrad Peukert, Lennart Wild, Christian Putensen, Sascha David, Christian Bode\",\"doi\":\"10.1186/s40635-025-00725-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sepsis and septic shock, defined by a profound immune dysregulation, are among the leading causes of death in the intensive care unit (ICU). Despite advances in understanding the underlying pathophysiology, evidence for specific immunomodulatory treatment does not exist to date. Therapeutic plasma exchange (TPE) represents an adjunctive treatment approach to rebalance immune homeostasis. In the EXCHANGE-1 trial, we recently demonstrated a rapid hemodynamic improvement, possibly caused by the removal of harmful mediators and the replacement of protective plasma proteins. The aim of this secondary analysis is to further characterize the underlying immunomodulatory effects and to identify biomarkers that may predict treatment response.</p><p><strong>Methods: </strong>This secondary analysis included patients in early septic shock (< 24 h duration) and a norepinephrine (NE) dose of ≥ 0.4 μg/kg/min. Patients were randomized 1:1 to receive standard of care (SOC) or SOC + one single TPE and plasma samples were collected before and after TPE. Within-group and between group effects of circulating levels of acute-phase proteins [CRP and Pentraxin3 (PTX3)], inflammatory mediators (IL-4, IL-6, IL-8, IL-10, TNF-α, IL-2Rα/CD25) and damage-associated molecular pattern (DAMP) [cell-free DNA (cfDNA)] were analyzed via paired t test or Wilcoxon signed-rank test and a mixed-effects model. Multivariate mixed-effects modeling of NE and lactate reduction was performed to investigate if cfDNA could be associated with treatment response to TPE.</p><p><strong>Results: </strong>TPE led to a significant reduction in circulating acute-phase protein levels (CRP p = 0.00976, PTX3 p = 0.0001). Pro-inflammatory cytokines, such as circulating TNF-α-, IL-6- und IL-8-levels, were significantly reduced in both groups with no significant difference between treatment groups except for IL-2Rα/CD25 (p ≤ 0.0001). In a multivariate mixed-effects model, rising cfDNA levels over the first 6 h indicated refractoriness to SOC treatment regarding NE (p = 0.004) and lactate (p = 0.001), whereas those receiving TPE demonstrated sustained reductions in both parameters.</p><p><strong>Conclusions: </strong>In this secondary analysis of the EXCHANGE-1 trial adjunctive TPE is associated with the reduction of acute-phase proteins and IL-2Rα/CD25, however not with the reduction of pro-inflammatory cytokines. This phenomenon could contribute to the observed enhancement in hemodynamics among patients with septic shock. Furthermore, TPE may be particularly beneficial for patients with septic shock who exhibit rising levels of cfDNA.</p>\",\"PeriodicalId\":13750,\"journal\":{\"name\":\"Intensive Care Medicine Experimental\",\"volume\":\"13 1\",\"pages\":\"18\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-02-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11828778/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Intensive Care Medicine Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40635-025-00725-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00725-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:脓毒症和脓毒性休克是重症监护病房(ICU)死亡的主要原因之一,由严重的免疫失调所定义。尽管在了解潜在的病理生理学方面取得了进展,但特异性免疫调节治疗的证据尚不存在。治疗性血浆交换(TPE)是一种辅助治疗方法来重新平衡免疫稳态。在EXCHANGE-1试验中,我们最近证明了血液动力学的快速改善,可能是由于去除有害介质和替代保护性血浆蛋白引起的。这一次要分析的目的是进一步表征潜在的免疫调节作用,并确定可能预测治疗反应的生物标志物。方法:该二次分析纳入了早期脓毒性休克患者(结果:TPE导致循环急性期蛋白水平显著降低(CRP p = 0.00976, PTX3 p = 0.0001)。两组促炎因子如循环TNF-α-、IL-6-、il -8水平均显著降低,除IL-2Rα/CD25水平外,两组间差异无统计学意义(p≤0.0001)。在一个多变量混合效应模型中,cfDNA水平在前6小时上升表明,在NE (p = 0.004)和乳酸(p = 0.001)方面,SOC治疗的难治性,而接受TPE治疗的患者两项参数均持续降低。结论:在EXCHANGE-1试验的二级分析中,辅助性TPE与急性期蛋白和IL-2Rα/CD25的减少有关,但与促炎细胞因子的减少无关。这一现象可能有助于观察到脓毒性休克患者血流动力学的增强。此外,TPE可能对cfDNA水平升高的脓毒性休克患者特别有益。
The effect of therapeutic plasma exchange on the inflammatory response in septic shock: a secondary analysis of the EXCHANGE-1 trial.
Background: Sepsis and septic shock, defined by a profound immune dysregulation, are among the leading causes of death in the intensive care unit (ICU). Despite advances in understanding the underlying pathophysiology, evidence for specific immunomodulatory treatment does not exist to date. Therapeutic plasma exchange (TPE) represents an adjunctive treatment approach to rebalance immune homeostasis. In the EXCHANGE-1 trial, we recently demonstrated a rapid hemodynamic improvement, possibly caused by the removal of harmful mediators and the replacement of protective plasma proteins. The aim of this secondary analysis is to further characterize the underlying immunomodulatory effects and to identify biomarkers that may predict treatment response.
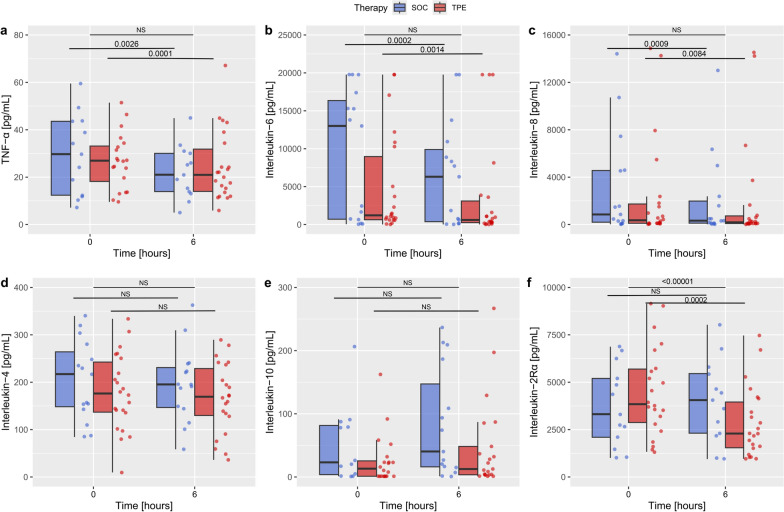
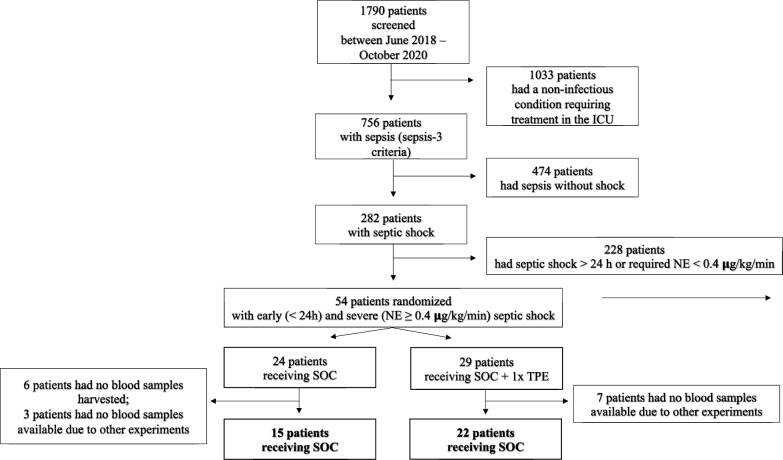
Methods: This secondary analysis included patients in early septic shock (< 24 h duration) and a norepinephrine (NE) dose of ≥ 0.4 μg/kg/min. Patients were randomized 1:1 to receive standard of care (SOC) or SOC + one single TPE and plasma samples were collected before and after TPE. Within-group and between group effects of circulating levels of acute-phase proteins [CRP and Pentraxin3 (PTX3)], inflammatory mediators (IL-4, IL-6, IL-8, IL-10, TNF-α, IL-2Rα/CD25) and damage-associated molecular pattern (DAMP) [cell-free DNA (cfDNA)] were analyzed via paired t test or Wilcoxon signed-rank test and a mixed-effects model. Multivariate mixed-effects modeling of NE and lactate reduction was performed to investigate if cfDNA could be associated with treatment response to TPE.
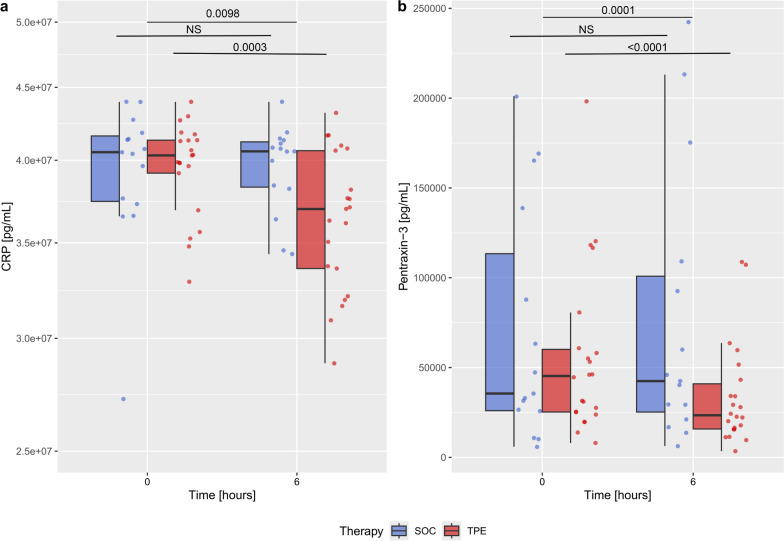
Results: TPE led to a significant reduction in circulating acute-phase protein levels (CRP p = 0.00976, PTX3 p = 0.0001). Pro-inflammatory cytokines, such as circulating TNF-α-, IL-6- und IL-8-levels, were significantly reduced in both groups with no significant difference between treatment groups except for IL-2Rα/CD25 (p ≤ 0.0001). In a multivariate mixed-effects model, rising cfDNA levels over the first 6 h indicated refractoriness to SOC treatment regarding NE (p = 0.004) and lactate (p = 0.001), whereas those receiving TPE demonstrated sustained reductions in both parameters.
Conclusions: In this secondary analysis of the EXCHANGE-1 trial adjunctive TPE is associated with the reduction of acute-phase proteins and IL-2Rα/CD25, however not with the reduction of pro-inflammatory cytokines. This phenomenon could contribute to the observed enhancement in hemodynamics among patients with septic shock. Furthermore, TPE may be particularly beneficial for patients with septic shock who exhibit rising levels of cfDNA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


