Nicolò Fabbri, Salvatore Greco, Antonio Pesce, Francesco Virgilio, Luca Bonazza, Luca Bagnoli, Carlo V Feo
{"title":"加强对急性胆囊炎和坏疽性胆囊炎的管理:由 TriNetX 数据库支持的系统性综述。","authors":"Nicolò Fabbri, Salvatore Greco, Antonio Pesce, Francesco Virgilio, Luca Bonazza, Luca Bagnoli, Carlo V Feo","doi":"10.21037/tgh-24-27","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute cholecystitis (AC) leads to emergency hospital admissions, and is categorized into mild, moderate, or severe grades, and affects hospital stay, surgery rates, costs, and prognosis. Gangrenous cholecystitis (GC) is the severe form and entails gallbladder wall necrosis and infection, possibly leading to emphysematous cholecystitis (EC), a life-threatening variant: early recognition of such a condition is crucial, since its symptoms may mimic uncomplicated AC. The current literature lacks comprehensive reviews on EC and GC due to their rarity and this study aims to bridge this gap by utilizing the TriNetX database, comparing clinical data of AC with GC outcomes.</p><p><strong>Methods: </strong>The study involved data retrieval from PubMed and Medline and the TriNetX database. Initially, 981 English articles were identified, focusing on emphysematous and GC and cholecystectomy. After filtering and reviewing, 73 articles were suitable for inclusion. We analyzed electronic medical records of adults diagnosed with AC, comparing demographics, comorbidities, and medications between medical and surgical intervention groups. Propensity score matching balanced cohorts, and Kaplan-Meier analysis estimated outcomes, while other statistical analyses, including risk ratios (RRs) and odds ratios (ORs), were conducted within TriNetX, with significance set at P<0.05. The study aimed to compare 5-year all-cause mortality in AC patients treated with or without surgery.</p><p><strong>Results: </strong>We found 9 retrospective studies and 3 prospective studies. Additionally, 70 patients from 62 case reports were utilized for descriptive analyses. From the TriNetX database, a total of 245,668 patients hospitalized for AC we identified. Despite, overweight/obesity was more frequent in the surgery group (24% <i>vs.</i> 14%, P<0.001), hypertension, diabetes mellitus, ischemic heart disease, chronic kidney disease and cerebrovascular diseases were more frequent in the non-operated patients (37% <i>vs.</i> 36%; 20% <i>vs.</i> 17%; 19% <i>vs.</i> 13%; 12% <i>vs.</i> 8%; 11% <i>vs.</i> 6%, respectively, all with P<0.001). The data concerning gastric medications are particularly eloquent, since 43% of operated patients were treated with such drugs versus 33% of non-operated subjects, before surgery (P<0.001). As for Kaplan-Meier analyses, patients who underwent surgery for AC presented generally lower mortality rates in the whole period of follow-up extended to 5 years (RR 0.415, 95% CI: 0.403-0.426; OR 0.364, 95% CI: 0.353-0.376; P<0.001) and this was particularly evident in the first 200 days of observation since index event.</p><p><strong>Conclusions: </strong>In GC, timely surgical intervention within 72-96 hours reduces complications, such as infections and hospital admissions. Laparoscopic surgery decreases intensive care unit (ICU) admissions and intra-abdominal abscesses. For AC, proton pump inhibitors (PPIs) seem to increase the risk of surgical intervention. In general, surgery is crucial for overall survival in the first 200 days of post-hospitalization. Anyway, confirmation through additional studies is needed.</p>","PeriodicalId":94362,"journal":{"name":"Translational gastroenterology and hepatology","volume":"10 ","pages":"16"},"PeriodicalIF":2.5000,"publicationDate":"2024-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11811563/pdf/","citationCount":"0","resultStr":"{\"title\":\"Enhancing the management of acute and gangrenous cholecystitis: a systematic review supported by the TriNetX database.\",\"authors\":\"Nicolò Fabbri, Salvatore Greco, Antonio Pesce, Francesco Virgilio, Luca Bonazza, Luca Bagnoli, Carlo V Feo\",\"doi\":\"10.21037/tgh-24-27\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute cholecystitis (AC) leads to emergency hospital admissions, and is categorized into mild, moderate, or severe grades, and affects hospital stay, surgery rates, costs, and prognosis. Gangrenous cholecystitis (GC) is the severe form and entails gallbladder wall necrosis and infection, possibly leading to emphysematous cholecystitis (EC), a life-threatening variant: early recognition of such a condition is crucial, since its symptoms may mimic uncomplicated AC. The current literature lacks comprehensive reviews on EC and GC due to their rarity and this study aims to bridge this gap by utilizing the TriNetX database, comparing clinical data of AC with GC outcomes.</p><p><strong>Methods: </strong>The study involved data retrieval from PubMed and Medline and the TriNetX database. Initially, 981 English articles were identified, focusing on emphysematous and GC and cholecystectomy. After filtering and reviewing, 73 articles were suitable for inclusion. We analyzed electronic medical records of adults diagnosed with AC, comparing demographics, comorbidities, and medications between medical and surgical intervention groups. Propensity score matching balanced cohorts, and Kaplan-Meier analysis estimated outcomes, while other statistical analyses, including risk ratios (RRs) and odds ratios (ORs), were conducted within TriNetX, with significance set at P<0.05. The study aimed to compare 5-year all-cause mortality in AC patients treated with or without surgery.</p><p><strong>Results: </strong>We found 9 retrospective studies and 3 prospective studies. Additionally, 70 patients from 62 case reports were utilized for descriptive analyses. From the TriNetX database, a total of 245,668 patients hospitalized for AC we identified. Despite, overweight/obesity was more frequent in the surgery group (24% <i>vs.</i> 14%, P<0.001), hypertension, diabetes mellitus, ischemic heart disease, chronic kidney disease and cerebrovascular diseases were more frequent in the non-operated patients (37% <i>vs.</i> 36%; 20% <i>vs.</i> 17%; 19% <i>vs.</i> 13%; 12% <i>vs.</i> 8%; 11% <i>vs.</i> 6%, respectively, all with P<0.001). The data concerning gastric medications are particularly eloquent, since 43% of operated patients were treated with such drugs versus 33% of non-operated subjects, before surgery (P<0.001). As for Kaplan-Meier analyses, patients who underwent surgery for AC presented generally lower mortality rates in the whole period of follow-up extended to 5 years (RR 0.415, 95% CI: 0.403-0.426; OR 0.364, 95% CI: 0.353-0.376; P<0.001) and this was particularly evident in the first 200 days of observation since index event.</p><p><strong>Conclusions: </strong>In GC, timely surgical intervention within 72-96 hours reduces complications, such as infections and hospital admissions. Laparoscopic surgery decreases intensive care unit (ICU) admissions and intra-abdominal abscesses. For AC, proton pump inhibitors (PPIs) seem to increase the risk of surgical intervention. In general, surgery is crucial for overall survival in the first 200 days of post-hospitalization. Anyway, confirmation through additional studies is needed.</p>\",\"PeriodicalId\":94362,\"journal\":{\"name\":\"Translational gastroenterology and hepatology\",\"volume\":\"10 \",\"pages\":\"16\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-11-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11811563/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational gastroenterology and hepatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/tgh-24-27\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/tgh-24-27","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:急性胆囊炎(AC)可导致急诊住院,分为轻度、中度或重度,并影响住院时间、手术率、费用和预后。坏疽性胆囊炎(GC)是一种严重的形式,包括胆囊壁坏死和感染,可能导致肺气肿性胆囊炎(EC),这是一种危及生命的变体:早期识别这种疾病至关重要,因为它的症状可能类似于简单的AC。由于EC和GC罕见,目前的文献缺乏全面的综述,本研究旨在通过利用TriNetX数据库,比较AC和GC的临床数据来弥补这一空白。方法:从PubMed、Medline和TriNetX数据库中检索数据。最初,确定了981篇英文文章,重点是肺气肿、GC和胆囊切除术。经过筛选和评审,有73篇文章适合纳入。我们分析了诊断为AC的成年人的电子医疗记录,比较了内科和外科干预组的人口统计学、合并症和药物治疗。倾向评分匹配平衡队列,Kaplan-Meier分析估计结果,而其他统计分析,包括风险比(rr)和优势比(ORs),在TriNetX中进行,显著性设置为结果:我们发现9项回顾性研究和3项前瞻性研究。此外,从62例病例报告中选取70例患者进行描述性分析。从TriNetX数据库中,我们共确定了245,668名因AC住院的患者。尽管如此,超重/肥胖在手术组更常见(24% vs. 14%, pv vs. 36%;20% vs. 17%;19% vs. 13%;12% vs. 8%;结论:在GC患者中,在72-96小时内及时进行手术干预可减少并发症,如感染和住院。腹腔镜手术减少重症监护病房(ICU)入院和腹腔内脓肿。对于AC,质子泵抑制剂(PPIs)似乎会增加手术干预的风险。一般来说,手术对住院后200天的总体生存率至关重要。无论如何,还需要进一步的研究来证实。
Enhancing the management of acute and gangrenous cholecystitis: a systematic review supported by the TriNetX database.
Background: Acute cholecystitis (AC) leads to emergency hospital admissions, and is categorized into mild, moderate, or severe grades, and affects hospital stay, surgery rates, costs, and prognosis. Gangrenous cholecystitis (GC) is the severe form and entails gallbladder wall necrosis and infection, possibly leading to emphysematous cholecystitis (EC), a life-threatening variant: early recognition of such a condition is crucial, since its symptoms may mimic uncomplicated AC. The current literature lacks comprehensive reviews on EC and GC due to their rarity and this study aims to bridge this gap by utilizing the TriNetX database, comparing clinical data of AC with GC outcomes.
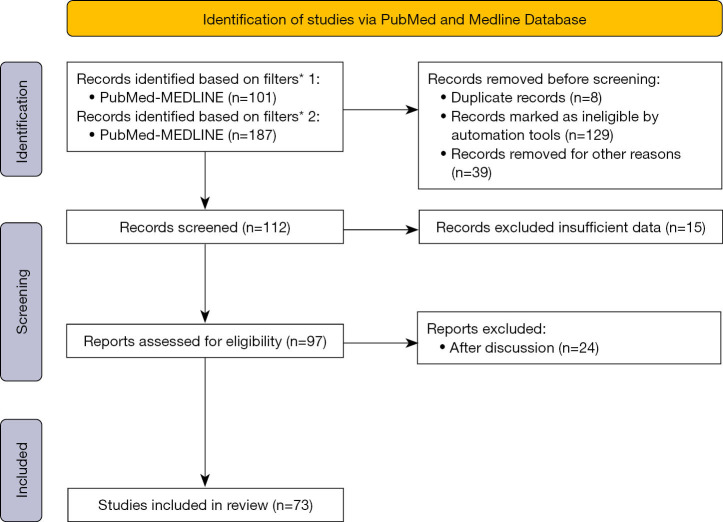
Methods: The study involved data retrieval from PubMed and Medline and the TriNetX database. Initially, 981 English articles were identified, focusing on emphysematous and GC and cholecystectomy. After filtering and reviewing, 73 articles were suitable for inclusion. We analyzed electronic medical records of adults diagnosed with AC, comparing demographics, comorbidities, and medications between medical and surgical intervention groups. Propensity score matching balanced cohorts, and Kaplan-Meier analysis estimated outcomes, while other statistical analyses, including risk ratios (RRs) and odds ratios (ORs), were conducted within TriNetX, with significance set at P<0.05. The study aimed to compare 5-year all-cause mortality in AC patients treated with or without surgery.
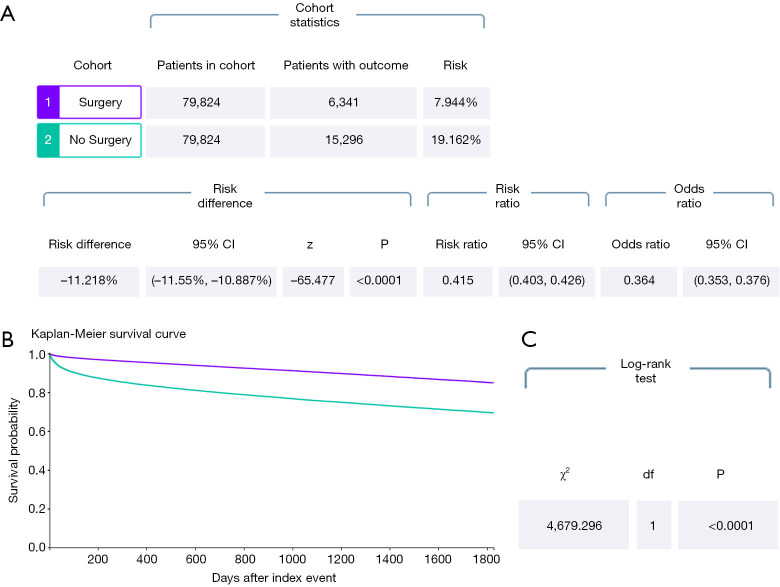
Results: We found 9 retrospective studies and 3 prospective studies. Additionally, 70 patients from 62 case reports were utilized for descriptive analyses. From the TriNetX database, a total of 245,668 patients hospitalized for AC we identified. Despite, overweight/obesity was more frequent in the surgery group (24% vs. 14%, P<0.001), hypertension, diabetes mellitus, ischemic heart disease, chronic kidney disease and cerebrovascular diseases were more frequent in the non-operated patients (37% vs. 36%; 20% vs. 17%; 19% vs. 13%; 12% vs. 8%; 11% vs. 6%, respectively, all with P<0.001). The data concerning gastric medications are particularly eloquent, since 43% of operated patients were treated with such drugs versus 33% of non-operated subjects, before surgery (P<0.001). As for Kaplan-Meier analyses, patients who underwent surgery for AC presented generally lower mortality rates in the whole period of follow-up extended to 5 years (RR 0.415, 95% CI: 0.403-0.426; OR 0.364, 95% CI: 0.353-0.376; P<0.001) and this was particularly evident in the first 200 days of observation since index event.
Conclusions: In GC, timely surgical intervention within 72-96 hours reduces complications, such as infections and hospital admissions. Laparoscopic surgery decreases intensive care unit (ICU) admissions and intra-abdominal abscesses. For AC, proton pump inhibitors (PPIs) seem to increase the risk of surgical intervention. In general, surgery is crucial for overall survival in the first 200 days of post-hospitalization. Anyway, confirmation through additional studies is needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


