{"title":"在日本进行的一项回顾性研究:在胰十二指肠切除术之前,超声引导下的原发性肝胃造口术用于胆道引流。","authors":"Nozomi Okuno, Kazuo Hara, Seiji Natsume, Masataka Okuno, Shin Haba, Tomonari Asano, Takamichi Kuwahara, Hiroki Koda, Yasuhiro Shimizu","doi":"10.5946/ce.2024.218","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Malignant lesions of the pancreatic head can cause obstructive jaundice requiring biliary drainage. However, the effect of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis and metal stents on surgical resection remains controversial. This study aimed to investigate the efficacy of primary endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) performed prior to pancreatoduodenectomy, excluding patients with biliary duct cancer.</p><p><strong>Methods: </strong>We retrospectively analyzed consecutive patients who underwent pancreatoduodenectomy at our institution between January 2019 and December 2022. The patients were divided into three groups: without biliary drainage (n=130), endoscopic biliary stenting (EBS) (n=57), and primary EUS-HGS (n=20).</p><p><strong>Results: </strong>The positivity rate of the intraoperative bile juice culture was significantly higher in the EBS group (p<0.001). No significant difference was observed among the groups in terms of postoperative adverse events (Clavien-Dindo grade 3 or higher, p=0.784) or the positive rate of peritoneal lavage cytology (p=0.984). Seven patients in the EBS group (12.3%) experienced early adverse events related to biliary drainage (post-ERCP pancreatitis, n=3; acute cholecystitis, n=3; bile duct perforation, n=1), whereas none in the EUS-HGS group experienced adverse events.</p><p><strong>Conclusions: </strong>Primary EUS-HGS is technically feasible as a preoperative procedure and has no short-term postoperative disadvantages.</p>","PeriodicalId":10351,"journal":{"name":"Clinical Endoscopy","volume":" ","pages":"604-611"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314625/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary endoscopic ultrasound-guided hepaticogastrostomy for biliary drainage prior to pancreatoduodenectomy: a retrospective study in Japan.\",\"authors\":\"Nozomi Okuno, Kazuo Hara, Seiji Natsume, Masataka Okuno, Shin Haba, Tomonari Asano, Takamichi Kuwahara, Hiroki Koda, Yasuhiro Shimizu\",\"doi\":\"10.5946/ce.2024.218\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Malignant lesions of the pancreatic head can cause obstructive jaundice requiring biliary drainage. However, the effect of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis and metal stents on surgical resection remains controversial. This study aimed to investigate the efficacy of primary endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) performed prior to pancreatoduodenectomy, excluding patients with biliary duct cancer.</p><p><strong>Methods: </strong>We retrospectively analyzed consecutive patients who underwent pancreatoduodenectomy at our institution between January 2019 and December 2022. The patients were divided into three groups: without biliary drainage (n=130), endoscopic biliary stenting (EBS) (n=57), and primary EUS-HGS (n=20).</p><p><strong>Results: </strong>The positivity rate of the intraoperative bile juice culture was significantly higher in the EBS group (p<0.001). No significant difference was observed among the groups in terms of postoperative adverse events (Clavien-Dindo grade 3 or higher, p=0.784) or the positive rate of peritoneal lavage cytology (p=0.984). Seven patients in the EBS group (12.3%) experienced early adverse events related to biliary drainage (post-ERCP pancreatitis, n=3; acute cholecystitis, n=3; bile duct perforation, n=1), whereas none in the EUS-HGS group experienced adverse events.</p><p><strong>Conclusions: </strong>Primary EUS-HGS is technically feasible as a preoperative procedure and has no short-term postoperative disadvantages.</p>\",\"PeriodicalId\":10351,\"journal\":{\"name\":\"Clinical Endoscopy\",\"volume\":\" \",\"pages\":\"604-611\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314625/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Endoscopy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5946/ce.2024.218\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5946/ce.2024.218","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Primary endoscopic ultrasound-guided hepaticogastrostomy for biliary drainage prior to pancreatoduodenectomy: a retrospective study in Japan.
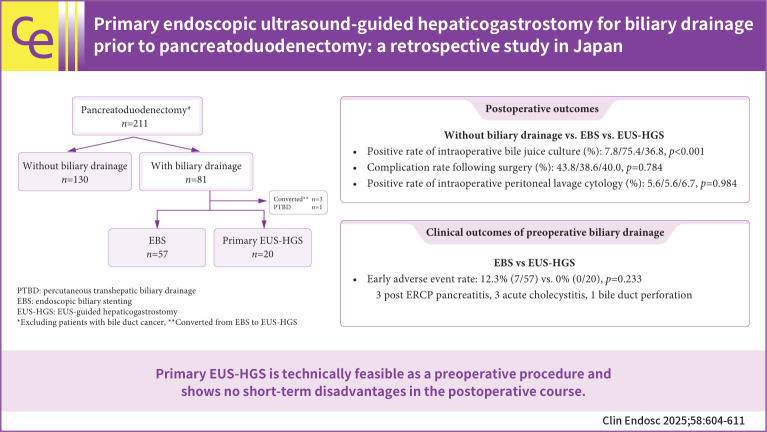
Background: Malignant lesions of the pancreatic head can cause obstructive jaundice requiring biliary drainage. However, the effect of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis and metal stents on surgical resection remains controversial. This study aimed to investigate the efficacy of primary endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) performed prior to pancreatoduodenectomy, excluding patients with biliary duct cancer.
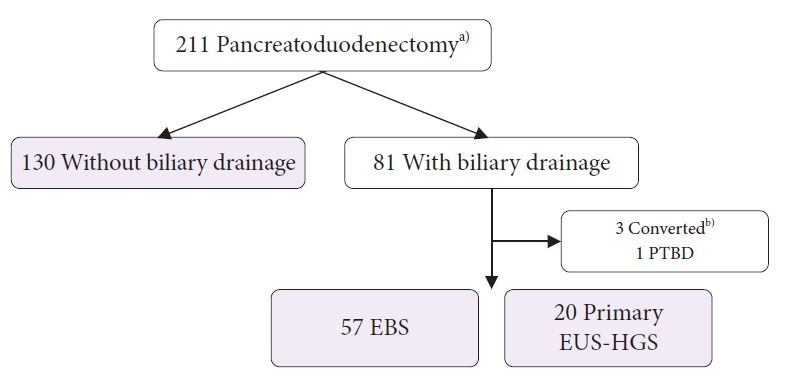
Methods: We retrospectively analyzed consecutive patients who underwent pancreatoduodenectomy at our institution between January 2019 and December 2022. The patients were divided into three groups: without biliary drainage (n=130), endoscopic biliary stenting (EBS) (n=57), and primary EUS-HGS (n=20).
Results: The positivity rate of the intraoperative bile juice culture was significantly higher in the EBS group (p<0.001). No significant difference was observed among the groups in terms of postoperative adverse events (Clavien-Dindo grade 3 or higher, p=0.784) or the positive rate of peritoneal lavage cytology (p=0.984). Seven patients in the EBS group (12.3%) experienced early adverse events related to biliary drainage (post-ERCP pancreatitis, n=3; acute cholecystitis, n=3; bile duct perforation, n=1), whereas none in the EUS-HGS group experienced adverse events.
Conclusions: Primary EUS-HGS is technically feasible as a preoperative procedure and has no short-term postoperative disadvantages.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


