Yishai Bachar Kirshenboim, Shir Tzur Lebovich, Tal Weitzer, Dana Doron, Moshe Bondi, Ron Cialic, Debbie Rand
{"title":"中风后上肢认知双任务能力。","authors":"Yishai Bachar Kirshenboim, Shir Tzur Lebovich, Tal Weitzer, Dana Doron, Moshe Bondi, Ron Cialic, Debbie Rand","doi":"10.1177/15459683251317192","DOIUrl":null,"url":null,"abstract":"<p><p>BackgroundDual-task capacity, which might be impaired poststroke, is needed for daily functions. Therefore, dual-task capacity should be assessed during rehabilitation. The Dual Overload Interference Test (DO-IT) is a new upper extremity (UE) protocol for assessment, combining The Box and Block Test with the Counting Backwards Test.ObjectivesTo validate DO-IT by comparing between (1) young and older healthy, (2) stroke and healthy participants. Additionally, to correlate DO-IT with (3) walking-cognitive dual-task assessment (healthy), and (4) standardized cognitive and EF assessments (stroke).MethodsA cross-sectional study included younger and older community-dwelling healthy individuals (N = 32), and younger and older individuals with stroke (N = 83). DO-IT was administered to all participants. The #blocks transferred (motor) and #correct numbers counted (cognitive) were recorded for single and dual conditions. The walking-cognitive dual-task test was administered to the healthy participants. Motor and cognitive costs were calculated as the difference between single and dual tasks. The Montreal Cognitive Assessment test (MoCA) and the Color Trail Test (CTT) assessed cognition post stroke.ResultsOlder healthy adults had significantly lower dual-task motor capacity compared to younger adults (median [interquartile range] blocks: older 26 [21-38], younger 46 [38-52], <i>P</i> < .01). Participants with stroke showed higher motor costs than healthy participants. Dual-task costs correlated between DO-IT to walking-cognitive (motor; <i>r</i> = .37-.41, cognitive; <i>r</i> = .41-.47, <i>P</i> < .05). DO-IT motor cost negatively correlated with MoCA (<i>r</i> = -.27, <i>P</i> < .05), and DO-IT motor performance correlated with MoCA/CTT-A\\B (<i>r</i> = .29-.60, <i>P</i> < .05).ConclusionsUE-Cognitive dual-task capacity is affected post-stroke. DO-IT shows potential for use in stroke rehabilitation and its validity should be further researched.</p>","PeriodicalId":94158,"journal":{"name":"Neurorehabilitation and neural repair","volume":" ","pages":"365-376"},"PeriodicalIF":3.7000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12065953/pdf/","citationCount":"0","resultStr":"{\"title\":\"Upper Extremity-Cognitive Dual-Task Capacity Post-Stroke.\",\"authors\":\"Yishai Bachar Kirshenboim, Shir Tzur Lebovich, Tal Weitzer, Dana Doron, Moshe Bondi, Ron Cialic, Debbie Rand\",\"doi\":\"10.1177/15459683251317192\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BackgroundDual-task capacity, which might be impaired poststroke, is needed for daily functions. Therefore, dual-task capacity should be assessed during rehabilitation. The Dual Overload Interference Test (DO-IT) is a new upper extremity (UE) protocol for assessment, combining The Box and Block Test with the Counting Backwards Test.ObjectivesTo validate DO-IT by comparing between (1) young and older healthy, (2) stroke and healthy participants. Additionally, to correlate DO-IT with (3) walking-cognitive dual-task assessment (healthy), and (4) standardized cognitive and EF assessments (stroke).MethodsA cross-sectional study included younger and older community-dwelling healthy individuals (N = 32), and younger and older individuals with stroke (N = 83). DO-IT was administered to all participants. The #blocks transferred (motor) and #correct numbers counted (cognitive) were recorded for single and dual conditions. The walking-cognitive dual-task test was administered to the healthy participants. Motor and cognitive costs were calculated as the difference between single and dual tasks. The Montreal Cognitive Assessment test (MoCA) and the Color Trail Test (CTT) assessed cognition post stroke.ResultsOlder healthy adults had significantly lower dual-task motor capacity compared to younger adults (median [interquartile range] blocks: older 26 [21-38], younger 46 [38-52], <i>P</i> < .01). Participants with stroke showed higher motor costs than healthy participants. Dual-task costs correlated between DO-IT to walking-cognitive (motor; <i>r</i> = .37-.41, cognitive; <i>r</i> = .41-.47, <i>P</i> < .05). DO-IT motor cost negatively correlated with MoCA (<i>r</i> = -.27, <i>P</i> < .05), and DO-IT motor performance correlated with MoCA/CTT-A\\\\B (<i>r</i> = .29-.60, <i>P</i> < .05).ConclusionsUE-Cognitive dual-task capacity is affected post-stroke. DO-IT shows potential for use in stroke rehabilitation and its validity should be further researched.</p>\",\"PeriodicalId\":94158,\"journal\":{\"name\":\"Neurorehabilitation and neural repair\",\"volume\":\" \",\"pages\":\"365-376\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12065953/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurorehabilitation and neural repair\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/15459683251317192\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurorehabilitation and neural repair","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/15459683251317192","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/11 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
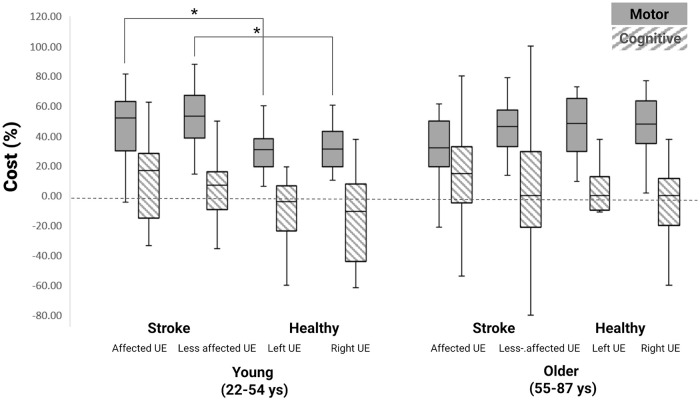
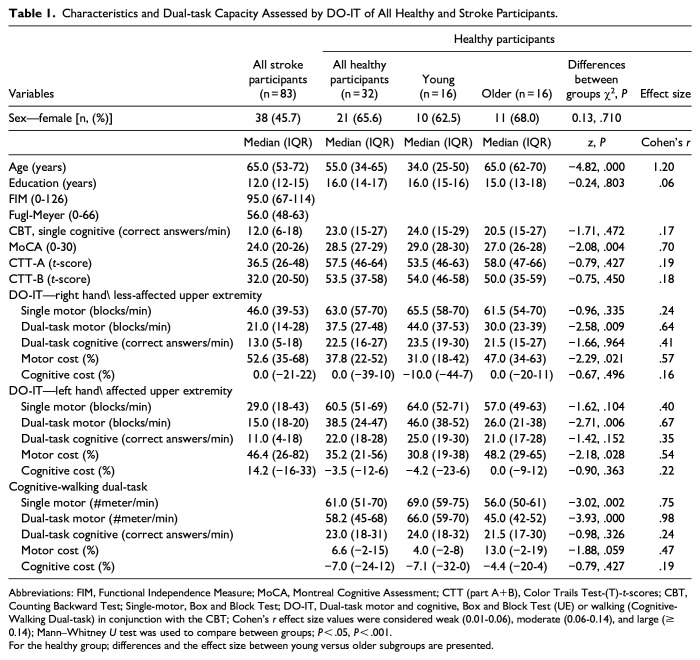
背景:脑卒中后,日常功能需要双任务能力,而这种能力可能会受损。因此,应在康复过程中对双任务能力进行评估。双过载干扰测试(DO-IT)是一种新的上肢(UE)评估方案,结合了箱块测试和倒数测试:通过比较(1)年轻和老年健康参与者,(2)中风和健康参与者,验证 DO-IT。此外,将 DO-IT 与(3)步行-认知双任务评估(健康)和(4)标准化认知和 EF 评估(脑卒中)相关联:一项横断面研究包括年轻和年长的社区健康人(32 人)以及年轻和年长的脑卒中患者(83 人)。所有参与者都进行了 DO-IT。记录了单一和双重条件下的块数转移(运动)和正确计数(认知)。对健康参与者进行了行走-认知双任务测试。运动和认知成本按单一任务和双重任务之间的差额计算。蒙特利尔认知评估测试(MoCA)和色彩轨迹测试(CTT)评估中风后的认知能力:结果:与年轻人相比,健康老年人的双任务运动能力明显较低(中位数[四分位数间距]块:老年人 26 [21-38],年轻人 46 [38-52],P r = .37-.41,认知能力;r = .41-.47,P r = -.27,P r = .29-.60,P 结论:老年人的双任务运动能力明显低于年轻人:UE-认知双任务能力在中风后会受到影响。DO-IT 显示了在脑卒中康复中使用的潜力,其有效性有待进一步研究。
BackgroundDual-task capacity, which might be impaired poststroke, is needed for daily functions. Therefore, dual-task capacity should be assessed during rehabilitation. The Dual Overload Interference Test (DO-IT) is a new upper extremity (UE) protocol for assessment, combining The Box and Block Test with the Counting Backwards Test.ObjectivesTo validate DO-IT by comparing between (1) young and older healthy, (2) stroke and healthy participants. Additionally, to correlate DO-IT with (3) walking-cognitive dual-task assessment (healthy), and (4) standardized cognitive and EF assessments (stroke).MethodsA cross-sectional study included younger and older community-dwelling healthy individuals (N = 32), and younger and older individuals with stroke (N = 83). DO-IT was administered to all participants. The #blocks transferred (motor) and #correct numbers counted (cognitive) were recorded for single and dual conditions. The walking-cognitive dual-task test was administered to the healthy participants. Motor and cognitive costs were calculated as the difference between single and dual tasks. The Montreal Cognitive Assessment test (MoCA) and the Color Trail Test (CTT) assessed cognition post stroke.ResultsOlder healthy adults had significantly lower dual-task motor capacity compared to younger adults (median [interquartile range] blocks: older 26 [21-38], younger 46 [38-52], P < .01). Participants with stroke showed higher motor costs than healthy participants. Dual-task costs correlated between DO-IT to walking-cognitive (motor; r = .37-.41, cognitive; r = .41-.47, P < .05). DO-IT motor cost negatively correlated with MoCA (r = -.27, P < .05), and DO-IT motor performance correlated with MoCA/CTT-A\B (r = .29-.60, P < .05).ConclusionsUE-Cognitive dual-task capacity is affected post-stroke. DO-IT shows potential for use in stroke rehabilitation and its validity should be further researched.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


