Syed M Adil, Tanner J Zachem, Jordan K Hatfield, Jihad Abdelgadir, Kimberly Hoang, Patrick J Codd
{"title":"锁眼小开颅中窝入路治疗腱鞘修复:病例系列及技术指导。","authors":"Syed M Adil, Tanner J Zachem, Jordan K Hatfield, Jihad Abdelgadir, Kimberly Hoang, Patrick J Codd","doi":"10.1055/a-2514-7338","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and Importance</b> Tegmen defects associated with cerebrospinal fluid (CSF) leaks are a rare pathology that can result in severe complications if left untreated. There is no universal optimal surgical algorithm for repair, although the most common techniques are the middle fossa craniotomy (traditionally 25 cm <sup>2</sup> in area), the transmastoid approach, or both. Here, we describe successful use of a keyhole mini-craniotomy, only 6 cm <sup>2</sup> in area, without mastoidectomy or days of lumbar drainage. <b>Clinical Presentation</b> Three patients presented with right-sided CSF otorrhea and hearing loss, with varying sizes of tegmen defects and associated encephaloceles. Keyhole craniotomies measuring 3 × 2 cm were used to perform a multilayer repair comprising an intradural collagen dural substitute, extradural fascial graft, extradural collagen dural substitute, fibrin sealant, and sometimes bony reconstruction using partial thickness craniotomy grafting. All patients were discharged on postoperative day 1 or 2, with no recurrence of symptoms at 6 months. <b>Conclusion</b> The keyhole craniotomy approach does not sacrifice the extent of operative access for this pathology. This minimally invasive approach can likely be used more often without need for concomitant mastoidectomy, ultimately enabling shorter hospital stays and more rapid recovery.</p>","PeriodicalId":44256,"journal":{"name":"Journal of Neurological Surgery Reports","volume":"86 1","pages":"e19-e23"},"PeriodicalIF":0.7000,"publicationDate":"2025-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11810456/pdf/","citationCount":"0","resultStr":"{\"title\":\"Keyhole Mini-Craniotomy Middle Fossa Approach for Tegmen Repair: A Case Series and Technical Instruction.\",\"authors\":\"Syed M Adil, Tanner J Zachem, Jordan K Hatfield, Jihad Abdelgadir, Kimberly Hoang, Patrick J Codd\",\"doi\":\"10.1055/a-2514-7338\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background and Importance</b> Tegmen defects associated with cerebrospinal fluid (CSF) leaks are a rare pathology that can result in severe complications if left untreated. There is no universal optimal surgical algorithm for repair, although the most common techniques are the middle fossa craniotomy (traditionally 25 cm <sup>2</sup> in area), the transmastoid approach, or both. Here, we describe successful use of a keyhole mini-craniotomy, only 6 cm <sup>2</sup> in area, without mastoidectomy or days of lumbar drainage. <b>Clinical Presentation</b> Three patients presented with right-sided CSF otorrhea and hearing loss, with varying sizes of tegmen defects and associated encephaloceles. Keyhole craniotomies measuring 3 × 2 cm were used to perform a multilayer repair comprising an intradural collagen dural substitute, extradural fascial graft, extradural collagen dural substitute, fibrin sealant, and sometimes bony reconstruction using partial thickness craniotomy grafting. All patients were discharged on postoperative day 1 or 2, with no recurrence of symptoms at 6 months. <b>Conclusion</b> The keyhole craniotomy approach does not sacrifice the extent of operative access for this pathology. This minimally invasive approach can likely be used more often without need for concomitant mastoidectomy, ultimately enabling shorter hospital stays and more rapid recovery.</p>\",\"PeriodicalId\":44256,\"journal\":{\"name\":\"Journal of Neurological Surgery Reports\",\"volume\":\"86 1\",\"pages\":\"e19-e23\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-02-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11810456/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurological Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2514-7338\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurological Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2514-7338","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Keyhole Mini-Craniotomy Middle Fossa Approach for Tegmen Repair: A Case Series and Technical Instruction.
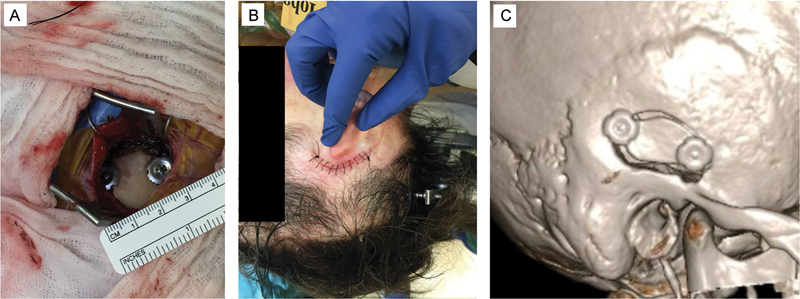
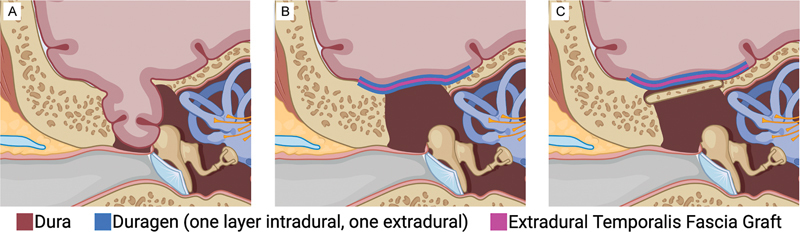
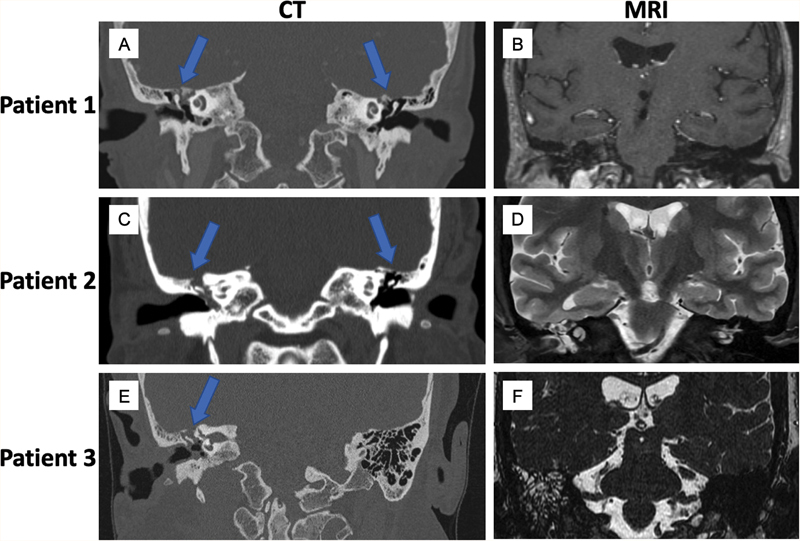
Background and Importance Tegmen defects associated with cerebrospinal fluid (CSF) leaks are a rare pathology that can result in severe complications if left untreated. There is no universal optimal surgical algorithm for repair, although the most common techniques are the middle fossa craniotomy (traditionally 25 cm 2 in area), the transmastoid approach, or both. Here, we describe successful use of a keyhole mini-craniotomy, only 6 cm 2 in area, without mastoidectomy or days of lumbar drainage. Clinical Presentation Three patients presented with right-sided CSF otorrhea and hearing loss, with varying sizes of tegmen defects and associated encephaloceles. Keyhole craniotomies measuring 3 × 2 cm were used to perform a multilayer repair comprising an intradural collagen dural substitute, extradural fascial graft, extradural collagen dural substitute, fibrin sealant, and sometimes bony reconstruction using partial thickness craniotomy grafting. All patients were discharged on postoperative day 1 or 2, with no recurrence of symptoms at 6 months. Conclusion The keyhole craniotomy approach does not sacrifice the extent of operative access for this pathology. This minimally invasive approach can likely be used more often without need for concomitant mastoidectomy, ultimately enabling shorter hospital stays and more rapid recovery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


