Lena Kretzschmar, Hubert Gabrys, Anja Joye, Johannes Kraft, Matthias Guckenberger, Nicolaus Andratschke
{"title":"脑转移瘤切除术后立体定向放疗(SRS)与低分割立体定向放疗(SRT) -单中心分析","authors":"Lena Kretzschmar, Hubert Gabrys, Anja Joye, Johannes Kraft, Matthias Guckenberger, Nicolaus Andratschke","doi":"10.1007/s10585-025-10334-5","DOIUrl":null,"url":null,"abstract":"<p><p>Postoperative radiotherapy improves local control (LC) after resection of brain metastases. In comparison to whole brain radiotherapy (WBRT) stereotactic radiosurgery (SRS) to resection cavity significantly reduces cognitive side effects. However, two phase-III trials have reported suboptimal LC with SRS, leading to increased interest in hypofractionated stereotactic radiotherapy (SRT) as an alternative to improve outcomes. This single-centre study, based on a prospective quality assurance protocol, included 161 patients with 185 resected brain metastases treated with either SRS or SRT between February 2018 and June 2023. Patients were assigned to treatment based on cavity size, with SRS typically used for cavities < 10 cc and SRT for larger volumes. Primary and secondary endpoints were LC and radiation necrosis (RN), respectively. Data analysis was conducted retrospectively. Median cavity size was 13.3 cc, with 20% of cavities receiving SRS and 80% SRT. 12-month LC was 92.6% (95-CI: 88.2 - 97.3%), 12-month RN incidence was 9% (95-CI: 3-14%), with RN limited to CTCAE v5 ≤ 2. In cavities < 10 cc, no significant difference in LC was found between SRS and SRT. For cavities > 10 cc, PTV volume was the only significant predictor of LC, while fractionation and dose did not significantly impact outcomes. SRS and SRT both offer excellent LC for resection cavities < 10 cc with low rates of RN, suggesting SRS as the preferred treatment in this collective, in consideration of patient comfort and resource allocation. In larger cavities, PTV volume significantly influences LC. Dose escalation might be beneficial in improving outcomes in these cases.</p>","PeriodicalId":10267,"journal":{"name":"Clinical & Experimental Metastasis","volume":"42 2","pages":"16"},"PeriodicalIF":3.2000,"publicationDate":"2025-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11811445/pdf/","citationCount":"0","resultStr":"{\"title\":\"Postoperative stereotactic radiosurgery (SRS) vs hypofractionated stereotactic radiotherapy (SRT) for resected brain metastases - a single centre analysis.\",\"authors\":\"Lena Kretzschmar, Hubert Gabrys, Anja Joye, Johannes Kraft, Matthias Guckenberger, Nicolaus Andratschke\",\"doi\":\"10.1007/s10585-025-10334-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Postoperative radiotherapy improves local control (LC) after resection of brain metastases. In comparison to whole brain radiotherapy (WBRT) stereotactic radiosurgery (SRS) to resection cavity significantly reduces cognitive side effects. However, two phase-III trials have reported suboptimal LC with SRS, leading to increased interest in hypofractionated stereotactic radiotherapy (SRT) as an alternative to improve outcomes. This single-centre study, based on a prospective quality assurance protocol, included 161 patients with 185 resected brain metastases treated with either SRS or SRT between February 2018 and June 2023. Patients were assigned to treatment based on cavity size, with SRS typically used for cavities < 10 cc and SRT for larger volumes. Primary and secondary endpoints were LC and radiation necrosis (RN), respectively. Data analysis was conducted retrospectively. Median cavity size was 13.3 cc, with 20% of cavities receiving SRS and 80% SRT. 12-month LC was 92.6% (95-CI: 88.2 - 97.3%), 12-month RN incidence was 9% (95-CI: 3-14%), with RN limited to CTCAE v5 ≤ 2. In cavities < 10 cc, no significant difference in LC was found between SRS and SRT. For cavities > 10 cc, PTV volume was the only significant predictor of LC, while fractionation and dose did not significantly impact outcomes. SRS and SRT both offer excellent LC for resection cavities < 10 cc with low rates of RN, suggesting SRS as the preferred treatment in this collective, in consideration of patient comfort and resource allocation. In larger cavities, PTV volume significantly influences LC. Dose escalation might be beneficial in improving outcomes in these cases.</p>\",\"PeriodicalId\":10267,\"journal\":{\"name\":\"Clinical & Experimental Metastasis\",\"volume\":\"42 2\",\"pages\":\"16\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-02-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11811445/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical & Experimental Metastasis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10585-025-10334-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical & Experimental Metastasis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10585-025-10334-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Postoperative stereotactic radiosurgery (SRS) vs hypofractionated stereotactic radiotherapy (SRT) for resected brain metastases - a single centre analysis.
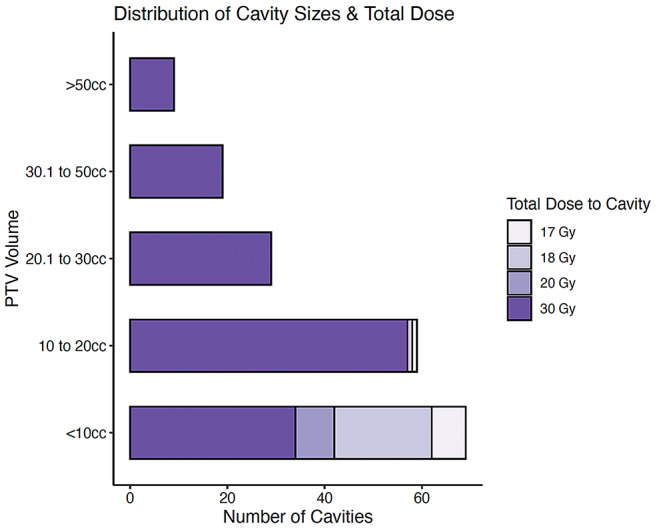
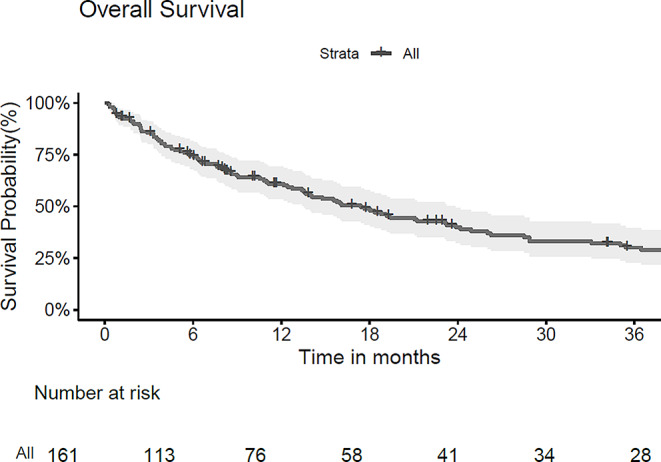
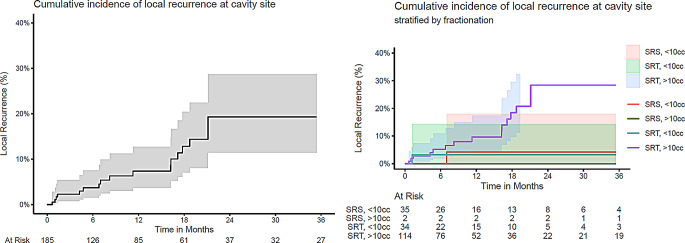
Postoperative radiotherapy improves local control (LC) after resection of brain metastases. In comparison to whole brain radiotherapy (WBRT) stereotactic radiosurgery (SRS) to resection cavity significantly reduces cognitive side effects. However, two phase-III trials have reported suboptimal LC with SRS, leading to increased interest in hypofractionated stereotactic radiotherapy (SRT) as an alternative to improve outcomes. This single-centre study, based on a prospective quality assurance protocol, included 161 patients with 185 resected brain metastases treated with either SRS or SRT between February 2018 and June 2023. Patients were assigned to treatment based on cavity size, with SRS typically used for cavities < 10 cc and SRT for larger volumes. Primary and secondary endpoints were LC and radiation necrosis (RN), respectively. Data analysis was conducted retrospectively. Median cavity size was 13.3 cc, with 20% of cavities receiving SRS and 80% SRT. 12-month LC was 92.6% (95-CI: 88.2 - 97.3%), 12-month RN incidence was 9% (95-CI: 3-14%), with RN limited to CTCAE v5 ≤ 2. In cavities < 10 cc, no significant difference in LC was found between SRS and SRT. For cavities > 10 cc, PTV volume was the only significant predictor of LC, while fractionation and dose did not significantly impact outcomes. SRS and SRT both offer excellent LC for resection cavities < 10 cc with low rates of RN, suggesting SRS as the preferred treatment in this collective, in consideration of patient comfort and resource allocation. In larger cavities, PTV volume significantly influences LC. Dose escalation might be beneficial in improving outcomes in these cases.
期刊介绍:
The Journal''s scope encompasses all aspects of metastasis research, whether laboratory-based, experimental or clinical and therapeutic. It covers such areas as molecular biology, pharmacology, tumor biology, and clinical cancer treatment (with all its subdivisions of surgery, chemotherapy and radio-therapy as well as pathology and epidemiology) insofar as these disciplines are concerned with the Journal''s core subject of metastasis formation, prevention and treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


