Takaaki Hasegawa, Masanori Mori, Takashi Yamaguchi, Kengo Imai, Yoshinobu Matsuda, Isseki Maeda, Yutaka Hatano, Naosuke Yokomichi, Jun Hamano, Tatsuya Morita, East Asian Collaborative Cross-Cultural Study to Elucidate the Dying Process (EASED) investigators
{"title":"为晚期呼吸困难患者提供谵妄缓解的药理学策略:一项次要数据分析","authors":"Takaaki Hasegawa, Masanori Mori, Takashi Yamaguchi, Kengo Imai, Yoshinobu Matsuda, Isseki Maeda, Yutaka Hatano, Naosuke Yokomichi, Jun Hamano, Tatsuya Morita, East Asian Collaborative Cross-Cultural Study to Elucidate the Dying Process (EASED) investigators","doi":"10.1002/cam4.70677","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Systemic opioids are recommended as a pharmacological treatment for dyspnea, and antipsychotics are widely used for delirium. Because little is known about optimal palliative pharmacological strategies for dyspnea in patients with delirium, this study explored the symptom course in such cases, including the use of opioids and antipsychotics.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a secondary analysis of a multicenter prospective and observational study. We consecutively enrolled adult patients with advanced cancer at palliative care units in Japan. The eligibility criteria for their participation were a dyspnea Integrated Palliative care Outcome Scale (IPOS) score ≥ 2 and the presence of delirium. We investigated pharmacological strategies, IPOS for dyspnea, and delirium symptoms using item 9 of the Memorial Delirium Assessment Scale.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of the 1896 patients, 141 were found eligible and were analyzed. Eighty-two (58%) patients had agitated delirium, and the median survival period was 4 days. Regarding pharmacological strategy, 31 (22%) received opioid initiation or dose escalation, whereas 92 (65%) used regular antipsychotics. Although mean dyspnea IPOS scores significantly decreased from Day 1 to Day 2 (0.44, 95% CI: 0.24–0.64), the proportion of responders (IPOS score ≤ 1) was 21% (30/141). In the agitated delirium group, the proportion of remaining agitation symptoms at Day 2 was 74% (61/82).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The combined distressing symptoms of dyspnea and delirium during the last days of life are likely to be refractory suffering, which shows a poor response to pharmacological interventions, including opioids and antipsychotics.</p>\n </section>\n </div>","PeriodicalId":139,"journal":{"name":"Cancer Medicine","volume":"14 3","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2025-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.70677","citationCount":"0","resultStr":"{\"title\":\"Pharmacological Strategies for Providing Patients With Delirium Relief From Terminal Dyspnea: A Secondary Data Analysis\",\"authors\":\"Takaaki Hasegawa, Masanori Mori, Takashi Yamaguchi, Kengo Imai, Yoshinobu Matsuda, Isseki Maeda, Yutaka Hatano, Naosuke Yokomichi, Jun Hamano, Tatsuya Morita, East Asian Collaborative Cross-Cultural Study to Elucidate the Dying Process (EASED) investigators\",\"doi\":\"10.1002/cam4.70677\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Systemic opioids are recommended as a pharmacological treatment for dyspnea, and antipsychotics are widely used for delirium. Because little is known about optimal palliative pharmacological strategies for dyspnea in patients with delirium, this study explored the symptom course in such cases, including the use of opioids and antipsychotics.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a secondary analysis of a multicenter prospective and observational study. We consecutively enrolled adult patients with advanced cancer at palliative care units in Japan. The eligibility criteria for their participation were a dyspnea Integrated Palliative care Outcome Scale (IPOS) score ≥ 2 and the presence of delirium. We investigated pharmacological strategies, IPOS for dyspnea, and delirium symptoms using item 9 of the Memorial Delirium Assessment Scale.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of the 1896 patients, 141 were found eligible and were analyzed. Eighty-two (58%) patients had agitated delirium, and the median survival period was 4 days. Regarding pharmacological strategy, 31 (22%) received opioid initiation or dose escalation, whereas 92 (65%) used regular antipsychotics. Although mean dyspnea IPOS scores significantly decreased from Day 1 to Day 2 (0.44, 95% CI: 0.24–0.64), the proportion of responders (IPOS score ≤ 1) was 21% (30/141). In the agitated delirium group, the proportion of remaining agitation symptoms at Day 2 was 74% (61/82).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>The combined distressing symptoms of dyspnea and delirium during the last days of life are likely to be refractory suffering, which shows a poor response to pharmacological interventions, including opioids and antipsychotics.</p>\\n </section>\\n </div>\",\"PeriodicalId\":139,\"journal\":{\"name\":\"Cancer Medicine\",\"volume\":\"14 3\",\"pages\":\"\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-02-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.70677\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70677\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70677","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Pharmacological Strategies for Providing Patients With Delirium Relief From Terminal Dyspnea: A Secondary Data Analysis
Introduction
Systemic opioids are recommended as a pharmacological treatment for dyspnea, and antipsychotics are widely used for delirium. Because little is known about optimal palliative pharmacological strategies for dyspnea in patients with delirium, this study explored the symptom course in such cases, including the use of opioids and antipsychotics.
Methods
This was a secondary analysis of a multicenter prospective and observational study. We consecutively enrolled adult patients with advanced cancer at palliative care units in Japan. The eligibility criteria for their participation were a dyspnea Integrated Palliative care Outcome Scale (IPOS) score ≥ 2 and the presence of delirium. We investigated pharmacological strategies, IPOS for dyspnea, and delirium symptoms using item 9 of the Memorial Delirium Assessment Scale.
Results
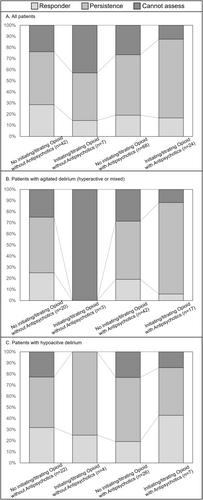
Of the 1896 patients, 141 were found eligible and were analyzed. Eighty-two (58%) patients had agitated delirium, and the median survival period was 4 days. Regarding pharmacological strategy, 31 (22%) received opioid initiation or dose escalation, whereas 92 (65%) used regular antipsychotics. Although mean dyspnea IPOS scores significantly decreased from Day 1 to Day 2 (0.44, 95% CI: 0.24–0.64), the proportion of responders (IPOS score ≤ 1) was 21% (30/141). In the agitated delirium group, the proportion of remaining agitation symptoms at Day 2 was 74% (61/82).
Conclusions
The combined distressing symptoms of dyspnea and delirium during the last days of life are likely to be refractory suffering, which shows a poor response to pharmacological interventions, including opioids and antipsychotics.
期刊介绍:
Cancer Medicine is a peer-reviewed, open access, interdisciplinary journal providing rapid publication of research from global biomedical researchers across the cancer sciences. The journal will consider submissions from all oncologic specialties, including, but not limited to, the following areas:
Clinical Cancer Research
Translational research ∙ clinical trials ∙ chemotherapy ∙ radiation therapy ∙ surgical therapy ∙ clinical observations ∙ clinical guidelines ∙ genetic consultation ∙ ethical considerations
Cancer Biology:
Molecular biology ∙ cellular biology ∙ molecular genetics ∙ genomics ∙ immunology ∙ epigenetics ∙ metabolic studies ∙ proteomics ∙ cytopathology ∙ carcinogenesis ∙ drug discovery and delivery.
Cancer Prevention:
Behavioral science ∙ psychosocial studies ∙ screening ∙ nutrition ∙ epidemiology and prevention ∙ community outreach.
Bioinformatics:
Gene expressions profiles ∙ gene regulation networks ∙ genome bioinformatics ∙ pathwayanalysis ∙ prognostic biomarkers.
Cancer Medicine publishes original research articles, systematic reviews, meta-analyses, and research methods papers, along with invited editorials and commentaries. Original research papers must report well-conducted research with conclusions supported by the data presented in the paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


