Jayastu Senapati, Sanam Loghavi, Jennifer Marvin-Peek, Guillermo Garcia-Manero, Tapan M. Kadia, Gautam Borthakur, Naval Daver, Nicholas J. Short, Nitin Jain, Ghayas C. Issa, Fadi Haddad, Danielle Hammond, Kelly Chien, Guillin Tang, Beenu Thakral, Guillermo Montalban-Bravo, Naveen Pemmaraju, Alexandre Bazinet, Mahesh Swaminathan, Sherry Pierce, Hussein A. Abbas, Patrick Reville, Uday Popat, Elizabeth Shpall, Richard Champlin, Elias Jabbour, Farhad Ravandi, Hagop M. Kantarjian, Courtney D. DiNardo
{"title":"继发性急性髓系白血病的临床-基因组研究:对当代治疗的反应和结果","authors":"Jayastu Senapati, Sanam Loghavi, Jennifer Marvin-Peek, Guillermo Garcia-Manero, Tapan M. Kadia, Gautam Borthakur, Naval Daver, Nicholas J. Short, Nitin Jain, Ghayas C. Issa, Fadi Haddad, Danielle Hammond, Kelly Chien, Guillin Tang, Beenu Thakral, Guillermo Montalban-Bravo, Naveen Pemmaraju, Alexandre Bazinet, Mahesh Swaminathan, Sherry Pierce, Hussein A. Abbas, Patrick Reville, Uday Popat, Elizabeth Shpall, Richard Champlin, Elias Jabbour, Farhad Ravandi, Hagop M. Kantarjian, Courtney D. DiNardo","doi":"10.1002/ajh.27628","DOIUrl":null,"url":null,"abstract":"<div>\n \n <p>Ontogeny of acute myeloid leukemia (AML) provides prognostic information, however closer interrogation with respect to AML characteristics, genomics, and various treatments are warranted. We defined untreated clinical secondary (CS) AML as AML with a diagnosis of antecedent myelodysplastic syndrome (MDS) or MDS/myeloproliferative neoplasm (MDS-MPN) without exposure to hypomethylating agents or chemotherapy; genomic secondary (GS) AML included patients with myelodysplasia related cytogenetics (MRC) or myelodysplasia related mutations (MRM) without a known antecedent myeloid neoplasm or prior chemo-radiotherapy for non-myeloid neoplasms. Among newly diagnosed AML patients classified as untreated CS-AML (<i>n</i> = 133) or GS-AML (<i>n</i> = 389), median relapse-free survival (RFS) (11.9 vs. 12.4 months, <i>p</i> = 0.36) and overall survival (OS) (11.6 vs. 14.4 months, <i>p</i> = 0.75) were similar. No difference in RFS and OS between these groups treated with low-intensity therapy (LIT) and venetoclax regimens was seen, but both were inferior to <i>de novo</i> (DN) AML without secondary-type genomics (pure DN-AML). GS-AML defined by the presence of only MRM had superior OS compared with MRM ± MRC with LIT+ venetoclax therapy (RFS 19.5 vs. 6.8 months [<i>p</i> < 0.01] and OS 29.6 vs. 8.4 [<i>p</i> < 0.01]) and had similar RFS (29.8 months, <i>p</i> = 0.48) and OS (32.0 months, <i>p</i> = 0.48) to pure DN-AML treated with LIT+ venetoclax. On multivariate analysis in patients treated with LIT+ venetoclax, untreated CS-AML (vs. GS-AML), adverse cytogenetics and ELN 2024 adverse-risk disease (mutated <i>TP53</i>) were associated with higher hazard of death. Adverse cytogenetics was the strongest prognostic variable predicting survival. Mutation-driven genomic ontogeny of newly diagnosed AML with MRM appears less prognostic than cytogenetic-driven ontogeny with venetoclax-based therapy.</p>\n </div>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"100 5","pages":"758-769"},"PeriodicalIF":10.1000,"publicationDate":"2025-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Clinico-Genomic Interrogation of Secondary-Type Acute Myeloid Leukemia: Response and Outcomes to Contemporary Therapies\",\"authors\":\"Jayastu Senapati, Sanam Loghavi, Jennifer Marvin-Peek, Guillermo Garcia-Manero, Tapan M. Kadia, Gautam Borthakur, Naval Daver, Nicholas J. Short, Nitin Jain, Ghayas C. Issa, Fadi Haddad, Danielle Hammond, Kelly Chien, Guillin Tang, Beenu Thakral, Guillermo Montalban-Bravo, Naveen Pemmaraju, Alexandre Bazinet, Mahesh Swaminathan, Sherry Pierce, Hussein A. Abbas, Patrick Reville, Uday Popat, Elizabeth Shpall, Richard Champlin, Elias Jabbour, Farhad Ravandi, Hagop M. Kantarjian, Courtney D. DiNardo\",\"doi\":\"10.1002/ajh.27628\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <p>Ontogeny of acute myeloid leukemia (AML) provides prognostic information, however closer interrogation with respect to AML characteristics, genomics, and various treatments are warranted. We defined untreated clinical secondary (CS) AML as AML with a diagnosis of antecedent myelodysplastic syndrome (MDS) or MDS/myeloproliferative neoplasm (MDS-MPN) without exposure to hypomethylating agents or chemotherapy; genomic secondary (GS) AML included patients with myelodysplasia related cytogenetics (MRC) or myelodysplasia related mutations (MRM) without a known antecedent myeloid neoplasm or prior chemo-radiotherapy for non-myeloid neoplasms. Among newly diagnosed AML patients classified as untreated CS-AML (<i>n</i> = 133) or GS-AML (<i>n</i> = 389), median relapse-free survival (RFS) (11.9 vs. 12.4 months, <i>p</i> = 0.36) and overall survival (OS) (11.6 vs. 14.4 months, <i>p</i> = 0.75) were similar. No difference in RFS and OS between these groups treated with low-intensity therapy (LIT) and venetoclax regimens was seen, but both were inferior to <i>de novo</i> (DN) AML without secondary-type genomics (pure DN-AML). GS-AML defined by the presence of only MRM had superior OS compared with MRM ± MRC with LIT+ venetoclax therapy (RFS 19.5 vs. 6.8 months [<i>p</i> < 0.01] and OS 29.6 vs. 8.4 [<i>p</i> < 0.01]) and had similar RFS (29.8 months, <i>p</i> = 0.48) and OS (32.0 months, <i>p</i> = 0.48) to pure DN-AML treated with LIT+ venetoclax. On multivariate analysis in patients treated with LIT+ venetoclax, untreated CS-AML (vs. GS-AML), adverse cytogenetics and ELN 2024 adverse-risk disease (mutated <i>TP53</i>) were associated with higher hazard of death. Adverse cytogenetics was the strongest prognostic variable predicting survival. Mutation-driven genomic ontogeny of newly diagnosed AML with MRM appears less prognostic than cytogenetic-driven ontogeny with venetoclax-based therapy.</p>\\n </div>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"100 5\",\"pages\":\"758-769\"},\"PeriodicalIF\":10.1000,\"publicationDate\":\"2025-02-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27628\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27628","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
急性髓性白血病(AML)的个体发生提供了预后信息,但是需要对AML的特征、基因组学和各种治疗方法进行更深入的研究。我们将未经治疗的临床继发性(CS) AML定义为诊断为既往骨髓增生异常综合征(MDS)或MDS/骨髓增生性肿瘤(MDS- mpn)的AML,未暴露于低甲基化药物或化疗;基因组继发性(GS) AML包括骨髓异常增生相关细胞遗传学(MRC)或骨髓异常增生相关突变(MRM)的患者,而没有已知的髓系肿瘤或既往的非髓系肿瘤化疗放疗。在新诊断的AML患者中,未治疗的CS-AML (n = 133)或GS-AML (n = 389),中位无复发生存期(RFS) (11.9 vs. 12.4个月,p = 0.36)和总生存期(OS) (11.6 vs. 14.4个月,p = 0.75)相似。低强度治疗(LIT)和venetoclax方案治疗组的RFS和OS没有差异,但两者都不如没有二级基因组学的新生(DN) AML(纯DN-AML)。仅MRM定义的GS-AML与MRM±MRC联合LIT+ venetoclax治疗相比具有更高的OS (RFS 19.5 vs. 6.8个月[p <; 0.01], OS 29.6 vs. 8.4 [p < 0.01]),并且与单纯的LIT+ venetoclax治疗的ns - aml具有相似的RFS(29.8个月,p = 0.48)和OS(32.0个月,p = 0.48)。在接受LIT+ venetoclax治疗的患者的多因素分析中,未经治疗的CS-AML (vs. GS-AML)、不良细胞遗传学和ELN 2024不良风险疾病(突变TP53)与更高的死亡风险相关。不良细胞遗传学是预测生存的最强预后变量。新诊断的AML伴MRM的突变驱动的基因组个体发生似乎比以venetoclax为基础的治疗的细胞遗传学驱动的个体发生的预后更差。
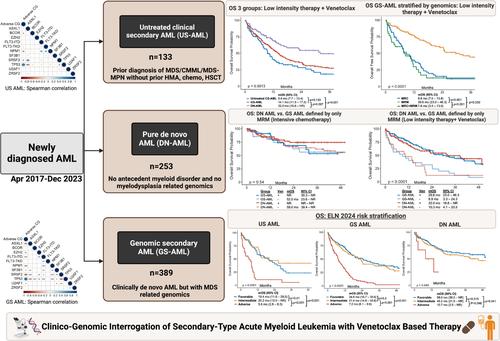
Clinico-Genomic Interrogation of Secondary-Type Acute Myeloid Leukemia: Response and Outcomes to Contemporary Therapies
Ontogeny of acute myeloid leukemia (AML) provides prognostic information, however closer interrogation with respect to AML characteristics, genomics, and various treatments are warranted. We defined untreated clinical secondary (CS) AML as AML with a diagnosis of antecedent myelodysplastic syndrome (MDS) or MDS/myeloproliferative neoplasm (MDS-MPN) without exposure to hypomethylating agents or chemotherapy; genomic secondary (GS) AML included patients with myelodysplasia related cytogenetics (MRC) or myelodysplasia related mutations (MRM) without a known antecedent myeloid neoplasm or prior chemo-radiotherapy for non-myeloid neoplasms. Among newly diagnosed AML patients classified as untreated CS-AML (n = 133) or GS-AML (n = 389), median relapse-free survival (RFS) (11.9 vs. 12.4 months, p = 0.36) and overall survival (OS) (11.6 vs. 14.4 months, p = 0.75) were similar. No difference in RFS and OS between these groups treated with low-intensity therapy (LIT) and venetoclax regimens was seen, but both were inferior to de novo (DN) AML without secondary-type genomics (pure DN-AML). GS-AML defined by the presence of only MRM had superior OS compared with MRM ± MRC with LIT+ venetoclax therapy (RFS 19.5 vs. 6.8 months [p < 0.01] and OS 29.6 vs. 8.4 [p < 0.01]) and had similar RFS (29.8 months, p = 0.48) and OS (32.0 months, p = 0.48) to pure DN-AML treated with LIT+ venetoclax. On multivariate analysis in patients treated with LIT+ venetoclax, untreated CS-AML (vs. GS-AML), adverse cytogenetics and ELN 2024 adverse-risk disease (mutated TP53) were associated with higher hazard of death. Adverse cytogenetics was the strongest prognostic variable predicting survival. Mutation-driven genomic ontogeny of newly diagnosed AML with MRM appears less prognostic than cytogenetic-driven ontogeny with venetoclax-based therapy.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


