Tareq Salous, Ryan Ashkar, Sandra K. Althouse, Clint Cary, Timothy Masterson, Nasser H. Hanna, Jennifer King, Lawrence H. Einhorn, Nabil Adra
{"title":"转移性生殖细胞瘤脑转移的预测模型","authors":"Tareq Salous, Ryan Ashkar, Sandra K. Althouse, Clint Cary, Timothy Masterson, Nasser H. Hanna, Jennifer King, Lawrence H. Einhorn, Nabil Adra","doi":"10.1002/cam4.70649","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Brain metastasis (BM) is an independent adverse prognostic factor in metastatic germ cell tumors (mGCT). We aimed to establish an effective and practical BM prediction model.</p>\n </section>\n \n <section>\n \n <h3> Patients and Methods</h3>\n \n <p>Between January 1990 and September 2017, 2291 patients with mGCT who were treated at Indiana University were identified. Patients were divided into two categories: BM present (<i>N</i> = 154) and BM absent (<i>N</i> = 2137). Kaplan–Meier methods were used to analyze progression free survival (PFS) and overall survival (OS). Logistic regression was used to determine a predictive model for whether BM was present. The data was separated into training and validation datasets with equal numbers of events in each.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The 2-year PFS and OS for patients with versus without BM: 17% versus 65% (<i>p</i> < 0.001) and 62% versus 91% (<i>p</i> < 0.001) respectively. Among the 154 patients with BM, 64 (42%) had radiation only (whole-brain radiotherapy or gamma knife), 22 (14%) had BM-surgery only, 14 (9%) had both radiation and BM-surgery. 54 patients (35%) did not receive local therapy for BM. Stepwise selection was used to determine the best model with <i>p</i> < 0.15 as the entry and staying criteria. The model with the largest ROC AUC was used moving forward. The model was tested in the validation dataset. A model was generated including age at diagnosis ≥ 40, choriocarcinoma predominant histology, pre-chemotherapy hCG≥ 5000, presence of pulmonary metastases size < 3, or ≥ 3 cm, and presence of bone metastasis. Patients with score of 0, 1, 2, 3, 4, 5, 6, 7, 8 points had a 0.6%, 1.4%, 3.5%, 8.2%, 18.3%, 36%, 58%, 78%, 90% probability of having BM, respectively.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The prediction model developed in this study demonstrated discrimination capability of predicting BM occurrence in mGCT and can be used to identify high-risk patients.</p>\n </section>\n </div>","PeriodicalId":139,"journal":{"name":"Cancer Medicine","volume":"14 3","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2025-02-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.70649","citationCount":"0","resultStr":"{\"title\":\"Prediction Model for Brain Metastasis in Patients With Metastatic Germ-Cell Tumors\",\"authors\":\"Tareq Salous, Ryan Ashkar, Sandra K. Althouse, Clint Cary, Timothy Masterson, Nasser H. Hanna, Jennifer King, Lawrence H. Einhorn, Nabil Adra\",\"doi\":\"10.1002/cam4.70649\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Brain metastasis (BM) is an independent adverse prognostic factor in metastatic germ cell tumors (mGCT). We aimed to establish an effective and practical BM prediction model.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Patients and Methods</h3>\\n \\n <p>Between January 1990 and September 2017, 2291 patients with mGCT who were treated at Indiana University were identified. Patients were divided into two categories: BM present (<i>N</i> = 154) and BM absent (<i>N</i> = 2137). Kaplan–Meier methods were used to analyze progression free survival (PFS) and overall survival (OS). Logistic regression was used to determine a predictive model for whether BM was present. The data was separated into training and validation datasets with equal numbers of events in each.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The 2-year PFS and OS for patients with versus without BM: 17% versus 65% (<i>p</i> < 0.001) and 62% versus 91% (<i>p</i> < 0.001) respectively. Among the 154 patients with BM, 64 (42%) had radiation only (whole-brain radiotherapy or gamma knife), 22 (14%) had BM-surgery only, 14 (9%) had both radiation and BM-surgery. 54 patients (35%) did not receive local therapy for BM. Stepwise selection was used to determine the best model with <i>p</i> < 0.15 as the entry and staying criteria. The model with the largest ROC AUC was used moving forward. The model was tested in the validation dataset. A model was generated including age at diagnosis ≥ 40, choriocarcinoma predominant histology, pre-chemotherapy hCG≥ 5000, presence of pulmonary metastases size < 3, or ≥ 3 cm, and presence of bone metastasis. Patients with score of 0, 1, 2, 3, 4, 5, 6, 7, 8 points had a 0.6%, 1.4%, 3.5%, 8.2%, 18.3%, 36%, 58%, 78%, 90% probability of having BM, respectively.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>The prediction model developed in this study demonstrated discrimination capability of predicting BM occurrence in mGCT and can be used to identify high-risk patients.</p>\\n </section>\\n </div>\",\"PeriodicalId\":139,\"journal\":{\"name\":\"Cancer Medicine\",\"volume\":\"14 3\",\"pages\":\"\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-02-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.70649\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70649\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70649","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Prediction Model for Brain Metastasis in Patients With Metastatic Germ-Cell Tumors
Background
Brain metastasis (BM) is an independent adverse prognostic factor in metastatic germ cell tumors (mGCT). We aimed to establish an effective and practical BM prediction model.
Patients and Methods
Between January 1990 and September 2017, 2291 patients with mGCT who were treated at Indiana University were identified. Patients were divided into two categories: BM present (N = 154) and BM absent (N = 2137). Kaplan–Meier methods were used to analyze progression free survival (PFS) and overall survival (OS). Logistic regression was used to determine a predictive model for whether BM was present. The data was separated into training and validation datasets with equal numbers of events in each.
Results
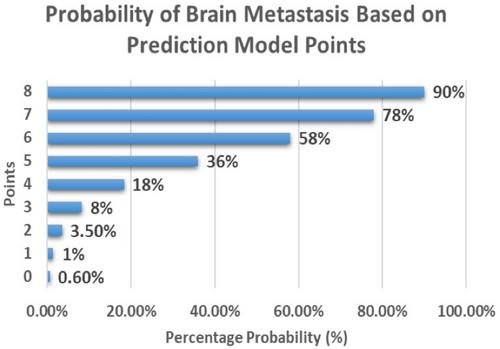
The 2-year PFS and OS for patients with versus without BM: 17% versus 65% (p < 0.001) and 62% versus 91% (p < 0.001) respectively. Among the 154 patients with BM, 64 (42%) had radiation only (whole-brain radiotherapy or gamma knife), 22 (14%) had BM-surgery only, 14 (9%) had both radiation and BM-surgery. 54 patients (35%) did not receive local therapy for BM. Stepwise selection was used to determine the best model with p < 0.15 as the entry and staying criteria. The model with the largest ROC AUC was used moving forward. The model was tested in the validation dataset. A model was generated including age at diagnosis ≥ 40, choriocarcinoma predominant histology, pre-chemotherapy hCG≥ 5000, presence of pulmonary metastases size < 3, or ≥ 3 cm, and presence of bone metastasis. Patients with score of 0, 1, 2, 3, 4, 5, 6, 7, 8 points had a 0.6%, 1.4%, 3.5%, 8.2%, 18.3%, 36%, 58%, 78%, 90% probability of having BM, respectively.
Conclusions
The prediction model developed in this study demonstrated discrimination capability of predicting BM occurrence in mGCT and can be used to identify high-risk patients.
期刊介绍:
Cancer Medicine is a peer-reviewed, open access, interdisciplinary journal providing rapid publication of research from global biomedical researchers across the cancer sciences. The journal will consider submissions from all oncologic specialties, including, but not limited to, the following areas:
Clinical Cancer Research
Translational research ∙ clinical trials ∙ chemotherapy ∙ radiation therapy ∙ surgical therapy ∙ clinical observations ∙ clinical guidelines ∙ genetic consultation ∙ ethical considerations
Cancer Biology:
Molecular biology ∙ cellular biology ∙ molecular genetics ∙ genomics ∙ immunology ∙ epigenetics ∙ metabolic studies ∙ proteomics ∙ cytopathology ∙ carcinogenesis ∙ drug discovery and delivery.
Cancer Prevention:
Behavioral science ∙ psychosocial studies ∙ screening ∙ nutrition ∙ epidemiology and prevention ∙ community outreach.
Bioinformatics:
Gene expressions profiles ∙ gene regulation networks ∙ genome bioinformatics ∙ pathwayanalysis ∙ prognostic biomarkers.
Cancer Medicine publishes original research articles, systematic reviews, meta-analyses, and research methods papers, along with invited editorials and commentaries. Original research papers must report well-conducted research with conclusions supported by the data presented in the paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


