Biche Osong, Eric Sribnick, Jonathan Groner, Rachel Stanley, Lauren Schulz, Bo Lu, Lawrence Cook, Henry Xiang
{"title":"使用人工智能建模为65岁以上的跌倒相关脑损伤患者提供临床决策支持。","authors":"Biche Osong, Eric Sribnick, Jonathan Groner, Rachel Stanley, Lauren Schulz, Bo Lu, Lawrence Cook, Henry Xiang","doi":"10.1371/journal.pone.0316462","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Older persons comprise most traumatic brain injury (TBI)-related hospitalizations and deaths and are particularly susceptible to fall-induced TBIs. The combination of increased frailty and susceptibility to clinical decline creates a significant ongoing challenge in the management of geriatric TBI. As the population ages and co-existing medical conditions complexify, so does the need to improve the quality of care for this population. Utilizing early hospital admission variables, this study will create and validate a multinomial decision tree that predicts the discharge disposition of older patients with fall-related TBI.</p><p><strong>Methods: </strong>From the National Trauma Data Bank, we retrospectively analyzed 11,977 older patients with a fall-related TBI (2017-2021). Clinical variables included Glasgow Coma Scale (GCS) score, intracranial pressure monitor use, venous thromboembolism (VTE) prophylaxis, and initial vital signs. Outcomes included hospital discharge disposition re-categorized into home, care facility, or deceased. Data were split into two sets, where 80% developed a decision tree, and 20% tested predictive performance. We employed a conditional inference tree algorithm with bootstrap (B = 100) and grid search options to grow the decision tree and measure discrimination ability using the area under the curve (AUC) and calibration plots.</p><p><strong>Results: </strong>Our decision tree used seven admission variables to predict the discharge disposition of older TBI patients. Significant non-modifiable variables included total GCS and injury severity scores, while VTE prophylaxis type was the most important interventional variable. Patients who did not receive VTE prophylaxis treatment had a higher probability of death. The predictive performance of the tree in terms of AUC value (95% confidence intervals) in the training cohort for death, care, and home were 0.66 (0.65-0.67), 0.75 (0.73-0.76), and 0.77 (0.76-0.79), respectively. In the test cohort, the values were 0.64 (0.62-0.67), 0.75 (0.72-0.77), and 0.77 (0.73-0.79).</p><p><strong>Conclusions: </strong>We have developed and internally validated a multinomial decision tree to predict the discharge destination of older patients with TBI. This tree could serve as a decision support tool for caregivers to manage older patients better and inform decision-making. However, the tree must be externally validated using prospective data to ascertain its predictive and clinical importance.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 2","pages":"e0316462"},"PeriodicalIF":2.6000,"publicationDate":"2025-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11790116/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development of clinical decision support for patients older than 65 years with fall-related TBI using artificial intelligence modeling.\",\"authors\":\"Biche Osong, Eric Sribnick, Jonathan Groner, Rachel Stanley, Lauren Schulz, Bo Lu, Lawrence Cook, Henry Xiang\",\"doi\":\"10.1371/journal.pone.0316462\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Older persons comprise most traumatic brain injury (TBI)-related hospitalizations and deaths and are particularly susceptible to fall-induced TBIs. The combination of increased frailty and susceptibility to clinical decline creates a significant ongoing challenge in the management of geriatric TBI. As the population ages and co-existing medical conditions complexify, so does the need to improve the quality of care for this population. Utilizing early hospital admission variables, this study will create and validate a multinomial decision tree that predicts the discharge disposition of older patients with fall-related TBI.</p><p><strong>Methods: </strong>From the National Trauma Data Bank, we retrospectively analyzed 11,977 older patients with a fall-related TBI (2017-2021). Clinical variables included Glasgow Coma Scale (GCS) score, intracranial pressure monitor use, venous thromboembolism (VTE) prophylaxis, and initial vital signs. Outcomes included hospital discharge disposition re-categorized into home, care facility, or deceased. Data were split into two sets, where 80% developed a decision tree, and 20% tested predictive performance. We employed a conditional inference tree algorithm with bootstrap (B = 100) and grid search options to grow the decision tree and measure discrimination ability using the area under the curve (AUC) and calibration plots.</p><p><strong>Results: </strong>Our decision tree used seven admission variables to predict the discharge disposition of older TBI patients. Significant non-modifiable variables included total GCS and injury severity scores, while VTE prophylaxis type was the most important interventional variable. Patients who did not receive VTE prophylaxis treatment had a higher probability of death. The predictive performance of the tree in terms of AUC value (95% confidence intervals) in the training cohort for death, care, and home were 0.66 (0.65-0.67), 0.75 (0.73-0.76), and 0.77 (0.76-0.79), respectively. In the test cohort, the values were 0.64 (0.62-0.67), 0.75 (0.72-0.77), and 0.77 (0.73-0.79).</p><p><strong>Conclusions: </strong>We have developed and internally validated a multinomial decision tree to predict the discharge destination of older patients with TBI. This tree could serve as a decision support tool for caregivers to manage older patients better and inform decision-making. However, the tree must be externally validated using prospective data to ascertain its predictive and clinical importance.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 2\",\"pages\":\"e0316462\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-02-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11790116/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0316462\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0316462","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Development of clinical decision support for patients older than 65 years with fall-related TBI using artificial intelligence modeling.
Background: Older persons comprise most traumatic brain injury (TBI)-related hospitalizations and deaths and are particularly susceptible to fall-induced TBIs. The combination of increased frailty and susceptibility to clinical decline creates a significant ongoing challenge in the management of geriatric TBI. As the population ages and co-existing medical conditions complexify, so does the need to improve the quality of care for this population. Utilizing early hospital admission variables, this study will create and validate a multinomial decision tree that predicts the discharge disposition of older patients with fall-related TBI.
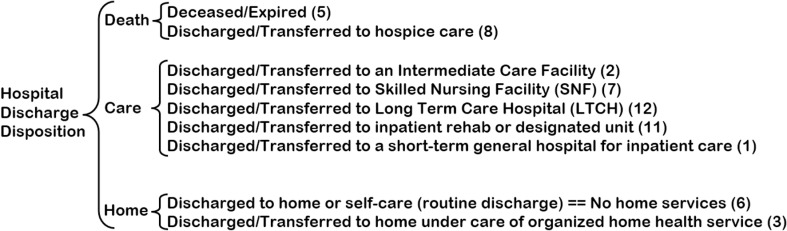
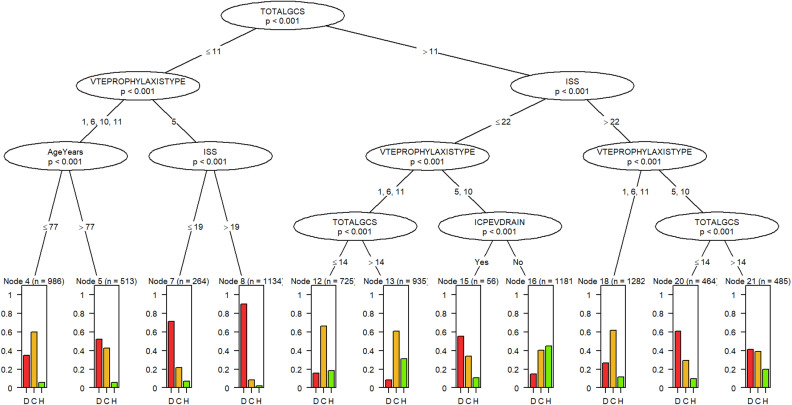
Methods: From the National Trauma Data Bank, we retrospectively analyzed 11,977 older patients with a fall-related TBI (2017-2021). Clinical variables included Glasgow Coma Scale (GCS) score, intracranial pressure monitor use, venous thromboembolism (VTE) prophylaxis, and initial vital signs. Outcomes included hospital discharge disposition re-categorized into home, care facility, or deceased. Data were split into two sets, where 80% developed a decision tree, and 20% tested predictive performance. We employed a conditional inference tree algorithm with bootstrap (B = 100) and grid search options to grow the decision tree and measure discrimination ability using the area under the curve (AUC) and calibration plots.
Results: Our decision tree used seven admission variables to predict the discharge disposition of older TBI patients. Significant non-modifiable variables included total GCS and injury severity scores, while VTE prophylaxis type was the most important interventional variable. Patients who did not receive VTE prophylaxis treatment had a higher probability of death. The predictive performance of the tree in terms of AUC value (95% confidence intervals) in the training cohort for death, care, and home were 0.66 (0.65-0.67), 0.75 (0.73-0.76), and 0.77 (0.76-0.79), respectively. In the test cohort, the values were 0.64 (0.62-0.67), 0.75 (0.72-0.77), and 0.77 (0.73-0.79).
Conclusions: We have developed and internally validated a multinomial decision tree to predict the discharge destination of older patients with TBI. This tree could serve as a decision support tool for caregivers to manage older patients better and inform decision-making. However, the tree must be externally validated using prospective data to ascertain its predictive and clinical importance.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


