Moritz T Huttelmaier, Alexander Gabel, Jonas Herting, Manuel Vogel, Stefan Störk, Stefan Frantz, Caroline Morbach, Thomas H Fischer
{"title":"以多极高密度接触测绘为特征的心房心肌病无创预测。","authors":"Moritz T Huttelmaier, Alexander Gabel, Jonas Herting, Manuel Vogel, Stefan Störk, Stefan Frantz, Caroline Morbach, Thomas H Fischer","doi":"10.1007/s10840-025-02001-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Atrial cardiomyopathy (AC) establishes links between atrial fibrillation (AF), left atrial (LA) mechanical dysfunction, structural remodeling, and thromboembolic events. Early diagnosis of AC may impact AF treatment and stroke risk prevention. Modern endocardial contact-mapping provides high-resolution electro-anatomical (EA) maps of the LA, thus allowing to display the myocardial substrate based on impaired signal amplitude and to characterize AC. Correlation of invasively assessed AC using a novel, multipolar mapping catheter (OCTARAY™, Biosense Webster, limited market release) and LA echocardiographic parameters could form the basis for a set of echo parameters for non-invasive prediction of AC.</p><p><strong>Methods: </strong>We retrospectively identified 50 adult patients who underwent primary pulmonary vein isolation (PVI) for paroxysmal or persistent AF between 08/22 and 05/23 fulfilling the selection criteria: (i) EA mapping with a novel multipolar mapping catheter (Octaray®); (ii) acquisition of voltage maps in sinus rhythm (SR) with ≥ 5000 points/map; and (iii) transthoracic echocardiography acquired in SR ≤ 48 h before PVI. Exclusion criterion was previous LA ablation. We generated EA maps with two sets of upper voltage thresholds (0.2-0.5 mV and 0.2-1.0 mV) and assessed total LA low voltage area (LVA). As LVA thresholds for the classification of AC are not yet established, an unsupervised machine learning cluster analysis was performed using a Gaussian mixture model (GMM), and two groups of patients with mild and severe AC were identified. Based on these two groups, we selected echo parameters for further analysis by applying the Boruta algorithm. The predictive capacity of the selected parameters was evaluated using a support vector machine.</p><p><strong>Results: </strong>The mean age of the studied sample (n = 50) was 63 ± 11 years, 62% were men, 64% showed persistent AF, median CHA<sub>2</sub>DS<sub>2</sub>-VASc score was 2 (quartiles 1, 3), and NT-proBNP was 190 (71, 391) pg/ml. A median of 5771 (5217, 6988) points/map were acquired. GMM yielded clusters of mild AC (n = 28) and severe AC (n = 22). Median LVA was 0.6 cm<sup>2</sup> (< 0.5 mV) resp. 4.1 cm<sup>2</sup> (< 1.0 mV) in group mild AC and 6.9 cm<sup>2</sup> (< 0.5 mV) resp. 27.2 cm<sup>2</sup> (< 1.0 mV) in group severe AC. Several echocardiographic parameters differed between the groups of mild and severe AC: dynamic LA parameters (end diastolic LA reservoir strain: 24.5% (22, 29) vs 15% (12, 19), p < 0.001; LA reservoir strain at atrial contraction: 22% (19, 25) vs 15% (11, 18), p < 0.001, end diastolic LA contraction strain: 13% (8, 15) vs 7.5% (3, 13), p < 0.01) as well as LA end-systolic volume index to a´ ratio (LAVI/a': 297 (231,365) vs 510 (326,781), p < 0.01). Consistent distribution of NT-proBNP (mild AC: 125 (48,189) pg/ml, severe AC: 408 (254,557) pg/ml, p < 0.0001) and CHA<sub>2</sub>DS<sub>2</sub>-VASc score (mild AC: 1 (1-2), severe AC: 3 (3-4), p < 0.0001) served as proof of concept. Applying the selected echocardiographic parameters, the machine learning algorithm correctly identified both subgroups with a mean AUC of 0.9 (95% CI 0.83-0.99). At 12 months, AF recurrence rate was 10.7% in mild AC and 40.9% in severe AC (p < 0.05).</p><p><strong>Conclusion: </strong>Among patients qualifying for PVI, machine learning analysis of high-resolution LA maps allowed to identify subgroups with mild and severe AC avoiding the use of arbitrary LVA thresholds. The subgroups were predicted non-invasively with good accuracy using a machine learning approach that incorporated a set of echocardiographic markers. This data could advance the clinical triage of patients with AF.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"865-876"},"PeriodicalIF":2.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12246000/pdf/","citationCount":"0","resultStr":"{\"title\":\"Non-invasive prediction of atrial cardiomyopathy characterized by multipolar high-density contact mapping.\",\"authors\":\"Moritz T Huttelmaier, Alexander Gabel, Jonas Herting, Manuel Vogel, Stefan Störk, Stefan Frantz, Caroline Morbach, Thomas H Fischer\",\"doi\":\"10.1007/s10840-025-02001-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Atrial cardiomyopathy (AC) establishes links between atrial fibrillation (AF), left atrial (LA) mechanical dysfunction, structural remodeling, and thromboembolic events. Early diagnosis of AC may impact AF treatment and stroke risk prevention. Modern endocardial contact-mapping provides high-resolution electro-anatomical (EA) maps of the LA, thus allowing to display the myocardial substrate based on impaired signal amplitude and to characterize AC. Correlation of invasively assessed AC using a novel, multipolar mapping catheter (OCTARAY™, Biosense Webster, limited market release) and LA echocardiographic parameters could form the basis for a set of echo parameters for non-invasive prediction of AC.</p><p><strong>Methods: </strong>We retrospectively identified 50 adult patients who underwent primary pulmonary vein isolation (PVI) for paroxysmal or persistent AF between 08/22 and 05/23 fulfilling the selection criteria: (i) EA mapping with a novel multipolar mapping catheter (Octaray®); (ii) acquisition of voltage maps in sinus rhythm (SR) with ≥ 5000 points/map; and (iii) transthoracic echocardiography acquired in SR ≤ 48 h before PVI. Exclusion criterion was previous LA ablation. We generated EA maps with two sets of upper voltage thresholds (0.2-0.5 mV and 0.2-1.0 mV) and assessed total LA low voltage area (LVA). As LVA thresholds for the classification of AC are not yet established, an unsupervised machine learning cluster analysis was performed using a Gaussian mixture model (GMM), and two groups of patients with mild and severe AC were identified. Based on these two groups, we selected echo parameters for further analysis by applying the Boruta algorithm. The predictive capacity of the selected parameters was evaluated using a support vector machine.</p><p><strong>Results: </strong>The mean age of the studied sample (n = 50) was 63 ± 11 years, 62% were men, 64% showed persistent AF, median CHA<sub>2</sub>DS<sub>2</sub>-VASc score was 2 (quartiles 1, 3), and NT-proBNP was 190 (71, 391) pg/ml. A median of 5771 (5217, 6988) points/map were acquired. GMM yielded clusters of mild AC (n = 28) and severe AC (n = 22). Median LVA was 0.6 cm<sup>2</sup> (< 0.5 mV) resp. 4.1 cm<sup>2</sup> (< 1.0 mV) in group mild AC and 6.9 cm<sup>2</sup> (< 0.5 mV) resp. 27.2 cm<sup>2</sup> (< 1.0 mV) in group severe AC. Several echocardiographic parameters differed between the groups of mild and severe AC: dynamic LA parameters (end diastolic LA reservoir strain: 24.5% (22, 29) vs 15% (12, 19), p < 0.001; LA reservoir strain at atrial contraction: 22% (19, 25) vs 15% (11, 18), p < 0.001, end diastolic LA contraction strain: 13% (8, 15) vs 7.5% (3, 13), p < 0.01) as well as LA end-systolic volume index to a´ ratio (LAVI/a': 297 (231,365) vs 510 (326,781), p < 0.01). Consistent distribution of NT-proBNP (mild AC: 125 (48,189) pg/ml, severe AC: 408 (254,557) pg/ml, p < 0.0001) and CHA<sub>2</sub>DS<sub>2</sub>-VASc score (mild AC: 1 (1-2), severe AC: 3 (3-4), p < 0.0001) served as proof of concept. Applying the selected echocardiographic parameters, the machine learning algorithm correctly identified both subgroups with a mean AUC of 0.9 (95% CI 0.83-0.99). At 12 months, AF recurrence rate was 10.7% in mild AC and 40.9% in severe AC (p < 0.05).</p><p><strong>Conclusion: </strong>Among patients qualifying for PVI, machine learning analysis of high-resolution LA maps allowed to identify subgroups with mild and severe AC avoiding the use of arbitrary LVA thresholds. The subgroups were predicted non-invasively with good accuracy using a machine learning approach that incorporated a set of echocardiographic markers. This data could advance the clinical triage of patients with AF.</p>\",\"PeriodicalId\":16202,\"journal\":{\"name\":\"Journal of Interventional Cardiac Electrophysiology\",\"volume\":\" \",\"pages\":\"865-876\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12246000/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Interventional Cardiac Electrophysiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10840-025-02001-2\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-025-02001-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Non-invasive prediction of atrial cardiomyopathy characterized by multipolar high-density contact mapping.
Introduction: Atrial cardiomyopathy (AC) establishes links between atrial fibrillation (AF), left atrial (LA) mechanical dysfunction, structural remodeling, and thromboembolic events. Early diagnosis of AC may impact AF treatment and stroke risk prevention. Modern endocardial contact-mapping provides high-resolution electro-anatomical (EA) maps of the LA, thus allowing to display the myocardial substrate based on impaired signal amplitude and to characterize AC. Correlation of invasively assessed AC using a novel, multipolar mapping catheter (OCTARAY™, Biosense Webster, limited market release) and LA echocardiographic parameters could form the basis for a set of echo parameters for non-invasive prediction of AC.
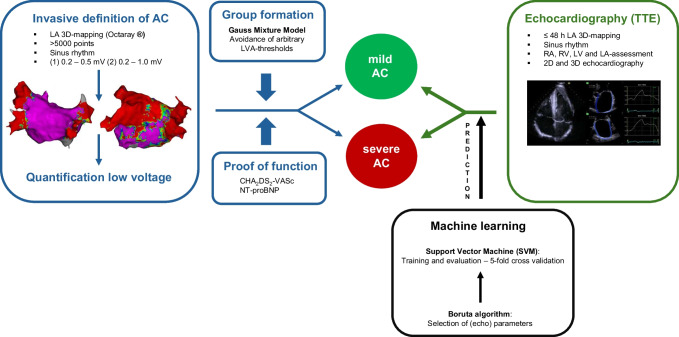
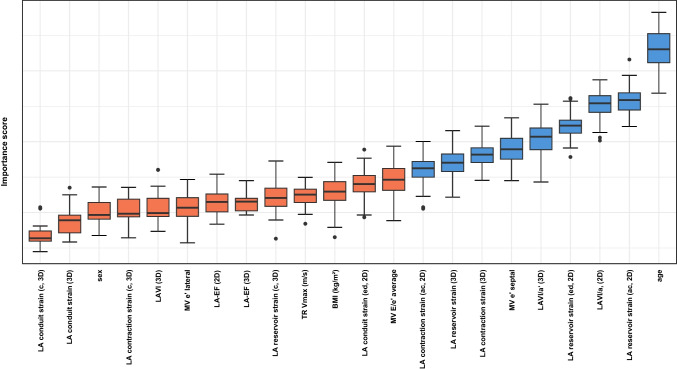
Methods: We retrospectively identified 50 adult patients who underwent primary pulmonary vein isolation (PVI) for paroxysmal or persistent AF between 08/22 and 05/23 fulfilling the selection criteria: (i) EA mapping with a novel multipolar mapping catheter (Octaray®); (ii) acquisition of voltage maps in sinus rhythm (SR) with ≥ 5000 points/map; and (iii) transthoracic echocardiography acquired in SR ≤ 48 h before PVI. Exclusion criterion was previous LA ablation. We generated EA maps with two sets of upper voltage thresholds (0.2-0.5 mV and 0.2-1.0 mV) and assessed total LA low voltage area (LVA). As LVA thresholds for the classification of AC are not yet established, an unsupervised machine learning cluster analysis was performed using a Gaussian mixture model (GMM), and two groups of patients with mild and severe AC were identified. Based on these two groups, we selected echo parameters for further analysis by applying the Boruta algorithm. The predictive capacity of the selected parameters was evaluated using a support vector machine.
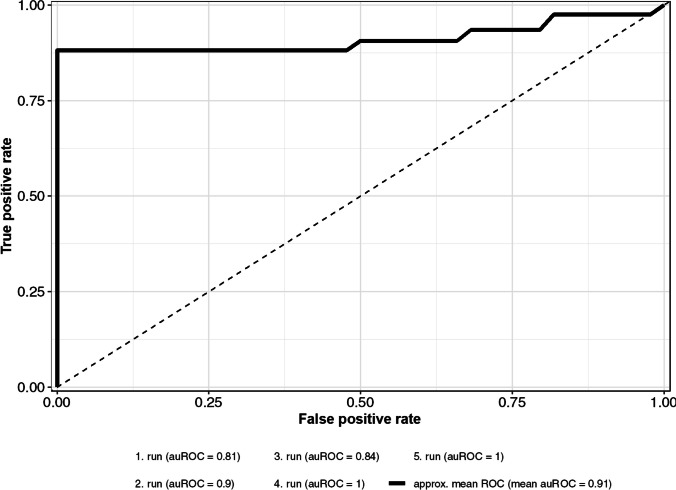
Results: The mean age of the studied sample (n = 50) was 63 ± 11 years, 62% were men, 64% showed persistent AF, median CHA2DS2-VASc score was 2 (quartiles 1, 3), and NT-proBNP was 190 (71, 391) pg/ml. A median of 5771 (5217, 6988) points/map were acquired. GMM yielded clusters of mild AC (n = 28) and severe AC (n = 22). Median LVA was 0.6 cm2 (< 0.5 mV) resp. 4.1 cm2 (< 1.0 mV) in group mild AC and 6.9 cm2 (< 0.5 mV) resp. 27.2 cm2 (< 1.0 mV) in group severe AC. Several echocardiographic parameters differed between the groups of mild and severe AC: dynamic LA parameters (end diastolic LA reservoir strain: 24.5% (22, 29) vs 15% (12, 19), p < 0.001; LA reservoir strain at atrial contraction: 22% (19, 25) vs 15% (11, 18), p < 0.001, end diastolic LA contraction strain: 13% (8, 15) vs 7.5% (3, 13), p < 0.01) as well as LA end-systolic volume index to a´ ratio (LAVI/a': 297 (231,365) vs 510 (326,781), p < 0.01). Consistent distribution of NT-proBNP (mild AC: 125 (48,189) pg/ml, severe AC: 408 (254,557) pg/ml, p < 0.0001) and CHA2DS2-VASc score (mild AC: 1 (1-2), severe AC: 3 (3-4), p < 0.0001) served as proof of concept. Applying the selected echocardiographic parameters, the machine learning algorithm correctly identified both subgroups with a mean AUC of 0.9 (95% CI 0.83-0.99). At 12 months, AF recurrence rate was 10.7% in mild AC and 40.9% in severe AC (p < 0.05).
Conclusion: Among patients qualifying for PVI, machine learning analysis of high-resolution LA maps allowed to identify subgroups with mild and severe AC avoiding the use of arbitrary LVA thresholds. The subgroups were predicted non-invasively with good accuracy using a machine learning approach that incorporated a set of echocardiographic markers. This data could advance the clinical triage of patients with AF.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


