Andreas Asheim, Sara Marie Nilsen, Signe Opdahl, Kari Risnes, Elisabeth Balstad Magnussen, Fredrik Carlsen, Neil Martin Davies, Johan Håkon Bjørngaard
{"title":"医院分娩量和出行时间对围产期死亡率和在途分娩的影响:基于三角剖分的因果推断。","authors":"Andreas Asheim, Sara Marie Nilsen, Signe Opdahl, Kari Risnes, Elisabeth Balstad Magnussen, Fredrik Carlsen, Neil Martin Davies, Johan Håkon Bjørngaard","doi":"10.1097/EDE.0000000000001840","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hospital regionalization involves balancing hospital volume and travel time. We investigated how hospital volume and travel time affect perinatal mortality and the risk of delivery in transit using three different study designs.</p><p><strong>Methods: </strong>This nationwide cohort study used data from the Medical Birth Registry of Norway (1999-2016) and Statistics Norway. We compared estimates across three designs: (1) Observed confounder adjustment: Comparing women giving birth at hospitals of different sizes and travel times (1,066,332 births), (2) Sibling comparison: Comparing women who moved between hospital catchment areas between births (203,464 births), and (3) Neighbor comparison: comparing women living in neighboring municipalities, but in different hospital catchment areas (460,776 births).</p><p><strong>Results: </strong>The study population included 5080 (0.48%) perinatal deaths and 7063 deliveries in transit (0.66%). For hospitals with 2000 compared with 500 births/year, observed confounder adjustment showed 1.81 times higher perinatal mortality (95% confidence interval [CI]: 1.21, 2.73). However, sibling and neighbor comparisons showed a factor of 0.64 (95% CI: 0.43, 0.97) and 0.61% (95% CI: 0.43, 0.88) lower perinatal mortality, respectively. Increased travel time was strongly associated with higher perinatal mortality using observed confounder adjustment, but this was not supported by the other designs. Longer travel time was consistently linked to an increased risk of delivery in transit.</p><p><strong>Conclusions: </strong>Perinatal mortality was higher in high-volume hospitals when adjusting for observed confounders. However, triangulating inferences from the other designs suggested the opposite, estimating that observed confounder control was insufficient. This supports the idea that access to higher-volume hospitals could improve perinatal outcomes at the population level.</p>","PeriodicalId":11779,"journal":{"name":"Epidemiology","volume":" ","pages":"425-435"},"PeriodicalIF":4.4000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11957439/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Effects of Hospital Delivery Volume and Travel Time on Perinatal Mortality and Delivery in Transit: Causal Inference with Triangulation.\",\"authors\":\"Andreas Asheim, Sara Marie Nilsen, Signe Opdahl, Kari Risnes, Elisabeth Balstad Magnussen, Fredrik Carlsen, Neil Martin Davies, Johan Håkon Bjørngaard\",\"doi\":\"10.1097/EDE.0000000000001840\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hospital regionalization involves balancing hospital volume and travel time. We investigated how hospital volume and travel time affect perinatal mortality and the risk of delivery in transit using three different study designs.</p><p><strong>Methods: </strong>This nationwide cohort study used data from the Medical Birth Registry of Norway (1999-2016) and Statistics Norway. We compared estimates across three designs: (1) Observed confounder adjustment: Comparing women giving birth at hospitals of different sizes and travel times (1,066,332 births), (2) Sibling comparison: Comparing women who moved between hospital catchment areas between births (203,464 births), and (3) Neighbor comparison: comparing women living in neighboring municipalities, but in different hospital catchment areas (460,776 births).</p><p><strong>Results: </strong>The study population included 5080 (0.48%) perinatal deaths and 7063 deliveries in transit (0.66%). For hospitals with 2000 compared with 500 births/year, observed confounder adjustment showed 1.81 times higher perinatal mortality (95% confidence interval [CI]: 1.21, 2.73). However, sibling and neighbor comparisons showed a factor of 0.64 (95% CI: 0.43, 0.97) and 0.61% (95% CI: 0.43, 0.88) lower perinatal mortality, respectively. Increased travel time was strongly associated with higher perinatal mortality using observed confounder adjustment, but this was not supported by the other designs. Longer travel time was consistently linked to an increased risk of delivery in transit.</p><p><strong>Conclusions: </strong>Perinatal mortality was higher in high-volume hospitals when adjusting for observed confounders. However, triangulating inferences from the other designs suggested the opposite, estimating that observed confounder control was insufficient. This supports the idea that access to higher-volume hospitals could improve perinatal outcomes at the population level.</p>\",\"PeriodicalId\":11779,\"journal\":{\"name\":\"Epidemiology\",\"volume\":\" \",\"pages\":\"425-435\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11957439/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/EDE.0000000000001840\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/EDE.0000000000001840","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/28 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
摘要
背景:医院区域化涉及到医院数量和出行时间的平衡。我们使用三种不同的研究设计调查了医院数量和出行时间如何影响围产期死亡率和途中分娩风险。方法:这项全国性队列研究使用了挪威医学出生登记处(1999-2016)和挪威统计局的数据。我们比较了三种设计的估计:(1)观察混杂因素调整:比较在不同规模和旅行时间的医院分娩的妇女(1,066,332例分娩);(2)兄弟姐妹比较:比较在医院集水区之间分娩的妇女(203,464例分娩);(3)邻居比较:比较居住在邻近城市但在不同医院集水区分娩的妇女(460,776例分娩)。结果:研究人群中围产期死亡5080例(0.48%),中转分娩7063例(0.66%)。与每年500名新生儿相比,2000名新生儿的医院,观察到的混杂因素调整显示围产期死亡率高出1.81倍(95%置信区间[CI] 1.21-2.73)。然而,兄弟姐妹和邻居比较显示围产儿死亡率分别降低0.64 (95% CI 0.43-0.97)和0.61% (95% CI 0.43-0.88)。使用观察到的混杂校正,增加的旅行时间与较高的围产期死亡率密切相关,但其他设计不支持这一点。较长的旅行时间一直与途中分娩的风险增加有关。结论:在调整观察到的混杂因素后,大容量医院的围产期死亡率更高。然而,从其他设计中得出的三角推断却显示出相反的结果,估计观察到的混杂因素控制是不够的。这支持了这样一种观点,即在人口水平上,进入规模较大的医院可以改善围产期结局。
The Effects of Hospital Delivery Volume and Travel Time on Perinatal Mortality and Delivery in Transit: Causal Inference with Triangulation.
Background: Hospital regionalization involves balancing hospital volume and travel time. We investigated how hospital volume and travel time affect perinatal mortality and the risk of delivery in transit using three different study designs.
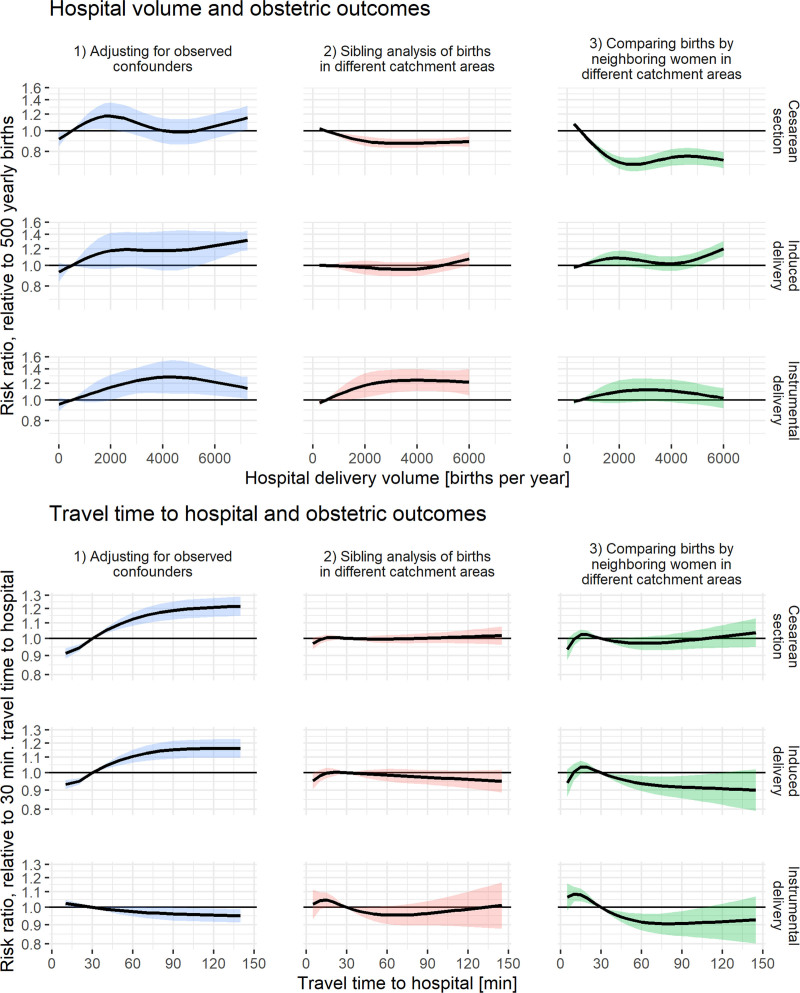
Methods: This nationwide cohort study used data from the Medical Birth Registry of Norway (1999-2016) and Statistics Norway. We compared estimates across three designs: (1) Observed confounder adjustment: Comparing women giving birth at hospitals of different sizes and travel times (1,066,332 births), (2) Sibling comparison: Comparing women who moved between hospital catchment areas between births (203,464 births), and (3) Neighbor comparison: comparing women living in neighboring municipalities, but in different hospital catchment areas (460,776 births).
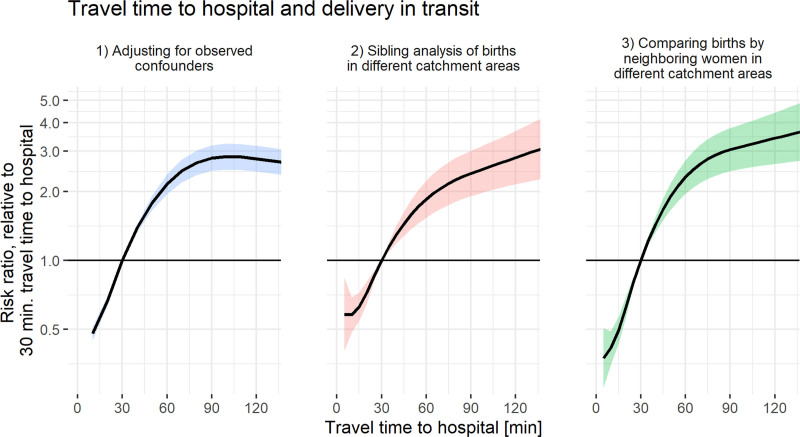
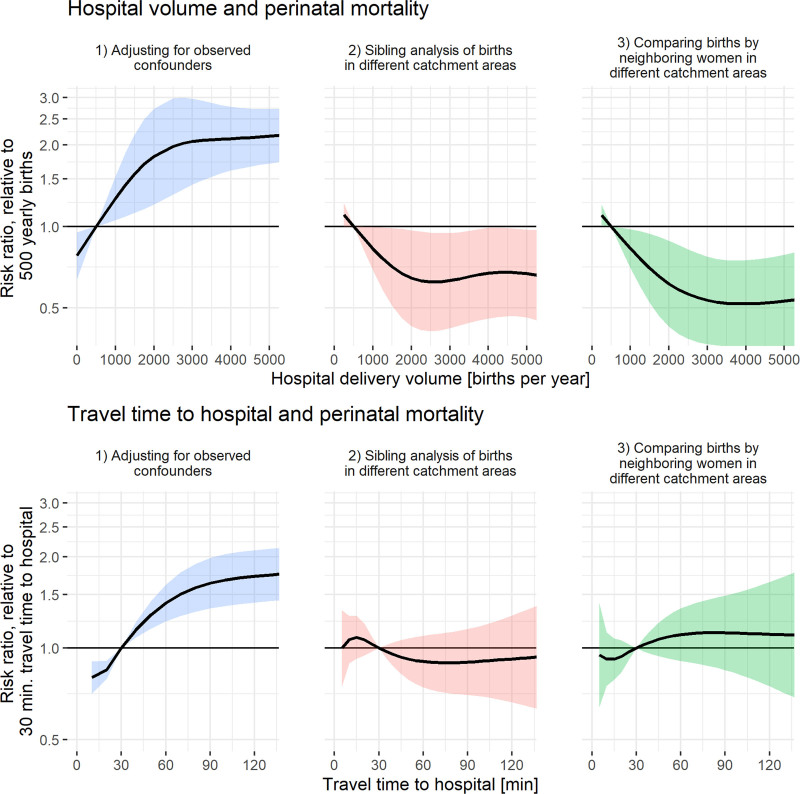
Results: The study population included 5080 (0.48%) perinatal deaths and 7063 deliveries in transit (0.66%). For hospitals with 2000 compared with 500 births/year, observed confounder adjustment showed 1.81 times higher perinatal mortality (95% confidence interval [CI]: 1.21, 2.73). However, sibling and neighbor comparisons showed a factor of 0.64 (95% CI: 0.43, 0.97) and 0.61% (95% CI: 0.43, 0.88) lower perinatal mortality, respectively. Increased travel time was strongly associated with higher perinatal mortality using observed confounder adjustment, but this was not supported by the other designs. Longer travel time was consistently linked to an increased risk of delivery in transit.
Conclusions: Perinatal mortality was higher in high-volume hospitals when adjusting for observed confounders. However, triangulating inferences from the other designs suggested the opposite, estimating that observed confounder control was insufficient. This supports the idea that access to higher-volume hospitals could improve perinatal outcomes at the population level.
期刊介绍:
Epidemiology publishes original research from all fields of epidemiology. The journal also welcomes review articles and meta-analyses, novel hypotheses, descriptions and applications of new methods, and discussions of research theory or public health policy. We give special consideration to papers from developing countries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


