Laibah Arshad Khan, Adeena Jamil, Stephen J Greene, Muhammad Shahzeb Khan, Javed Butler
{"title":"心力衰竭中的醛固酮和钾:克服临床实践中的这一主要障碍。","authors":"Laibah Arshad Khan, Adeena Jamil, Stephen J Greene, Muhammad Shahzeb Khan, Javed Butler","doi":"10.15420/cfr.2024.09","DOIUrl":null,"url":null,"abstract":"<p><p>Aldosterone is a key regulator of fluid and electrolyte balance in the body. It is often dysregulated in heart failure (HF) and is a key driver of cardiac remodelling and worse clinical outcomes. Potassium regulation is essential for normal cardiac, gastrointestinal and neuromuscular function. Serum potassium fluctuations are largely determined by aldosterone, the final step of the renin-angiotensin-aldosterone system. Dyskalaemia (i.e. hypokalaemia and hyperkalaemia) is prevalent in HF because of the disease itself, its therapies and related comorbidities such as chronic kidney disease. Prognostic implications of abnormal serum potassium follow a U-shaped curve, where both hypokalaemia and hyperkalaemia are associated with adverse outcomes. Hypokalaemia is associated with increased mortality, starting from potassium <4.0 mmol/l but especially at potassium <3.5 mmol/l. Hyperkalaemia, along with increasing arrhythmia risk, limits the use of lifesaving renin-angiotensin- aldosterone system inhibitors, which may have long-term survival implications. The advent of novel potassium binders aims to manage chronic hyperkalaemia and may allow for uptitration and optimal dosing of guideline-recommended therapy. This review discusses the impacts of dyskalaemia in HF, along with management strategies, including the relevance of potassium binder use in optimising HF treatment. Current and potential future aldosterone-modulating therapies, such as non-steroidal mineralocorticoid receptor antagonists and aldosterone synthase inhibitors, are also discussed.</p>","PeriodicalId":33741,"journal":{"name":"Cardiac Failure Review","volume":"10 ","pages":"e18"},"PeriodicalIF":5.7000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11770538/pdf/","citationCount":"0","resultStr":"{\"title\":\"Aldosterone and Potassium in Heart Failure: Overcoming This Major Impediment in Clinical Practice.\",\"authors\":\"Laibah Arshad Khan, Adeena Jamil, Stephen J Greene, Muhammad Shahzeb Khan, Javed Butler\",\"doi\":\"10.15420/cfr.2024.09\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Aldosterone is a key regulator of fluid and electrolyte balance in the body. It is often dysregulated in heart failure (HF) and is a key driver of cardiac remodelling and worse clinical outcomes. Potassium regulation is essential for normal cardiac, gastrointestinal and neuromuscular function. Serum potassium fluctuations are largely determined by aldosterone, the final step of the renin-angiotensin-aldosterone system. Dyskalaemia (i.e. hypokalaemia and hyperkalaemia) is prevalent in HF because of the disease itself, its therapies and related comorbidities such as chronic kidney disease. Prognostic implications of abnormal serum potassium follow a U-shaped curve, where both hypokalaemia and hyperkalaemia are associated with adverse outcomes. Hypokalaemia is associated with increased mortality, starting from potassium <4.0 mmol/l but especially at potassium <3.5 mmol/l. Hyperkalaemia, along with increasing arrhythmia risk, limits the use of lifesaving renin-angiotensin- aldosterone system inhibitors, which may have long-term survival implications. The advent of novel potassium binders aims to manage chronic hyperkalaemia and may allow for uptitration and optimal dosing of guideline-recommended therapy. This review discusses the impacts of dyskalaemia in HF, along with management strategies, including the relevance of potassium binder use in optimising HF treatment. Current and potential future aldosterone-modulating therapies, such as non-steroidal mineralocorticoid receptor antagonists and aldosterone synthase inhibitors, are also discussed.</p>\",\"PeriodicalId\":33741,\"journal\":{\"name\":\"Cardiac Failure Review\",\"volume\":\"10 \",\"pages\":\"e18\"},\"PeriodicalIF\":5.7000,\"publicationDate\":\"2024-12-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11770538/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiac Failure Review\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15420/cfr.2024.09\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiac Failure Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/cfr.2024.09","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Aldosterone and Potassium in Heart Failure: Overcoming This Major Impediment in Clinical Practice.
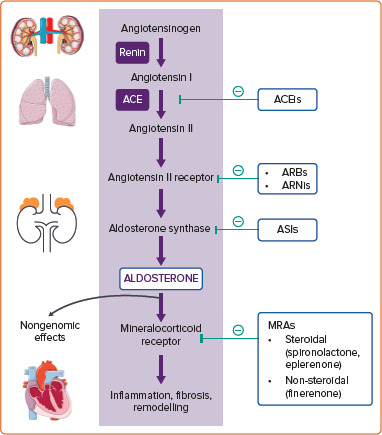
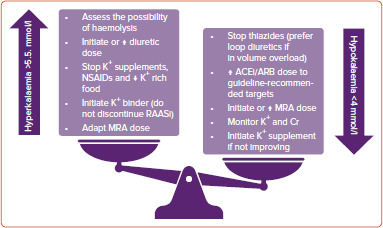
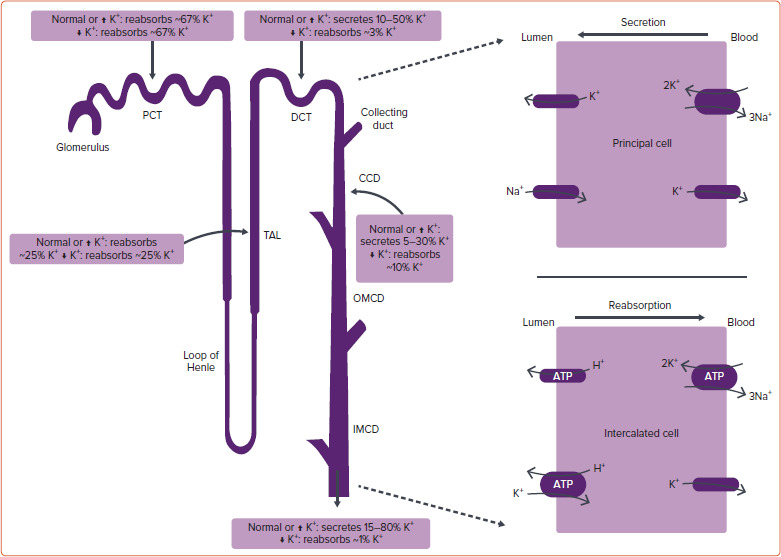
Aldosterone is a key regulator of fluid and electrolyte balance in the body. It is often dysregulated in heart failure (HF) and is a key driver of cardiac remodelling and worse clinical outcomes. Potassium regulation is essential for normal cardiac, gastrointestinal and neuromuscular function. Serum potassium fluctuations are largely determined by aldosterone, the final step of the renin-angiotensin-aldosterone system. Dyskalaemia (i.e. hypokalaemia and hyperkalaemia) is prevalent in HF because of the disease itself, its therapies and related comorbidities such as chronic kidney disease. Prognostic implications of abnormal serum potassium follow a U-shaped curve, where both hypokalaemia and hyperkalaemia are associated with adverse outcomes. Hypokalaemia is associated with increased mortality, starting from potassium <4.0 mmol/l but especially at potassium <3.5 mmol/l. Hyperkalaemia, along with increasing arrhythmia risk, limits the use of lifesaving renin-angiotensin- aldosterone system inhibitors, which may have long-term survival implications. The advent of novel potassium binders aims to manage chronic hyperkalaemia and may allow for uptitration and optimal dosing of guideline-recommended therapy. This review discusses the impacts of dyskalaemia in HF, along with management strategies, including the relevance of potassium binder use in optimising HF treatment. Current and potential future aldosterone-modulating therapies, such as non-steroidal mineralocorticoid receptor antagonists and aldosterone synthase inhibitors, are also discussed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


