{"title":"渗透性脱髓鞘综合征在正常血症背景下:1例报告和文献复习。","authors":"Rose V Zach, Jeffrey F Barletta, Victor Zach","doi":"10.1155/crnm/6626539","DOIUrl":null,"url":null,"abstract":"<p><p>Osmotic demyelination syndrome (ODS) is a rare complication associated with rapid sodium changes, typically encountered in patients with severe hyponatremia. ODS in patients with normonatremia (ODSIN) is less recognized. We describe a patient with MRI-detected ODSIN following neurotrauma and reviewed the relevant literature. We present a 57-year-old female with subdural hematoma following ground-level fall. Her initial sodium was 140 mEq/L but over 2 days, rose 17 mEq/L, peaking at 157 mEq/L. On exam, unexplainable, unexpected left-sided hemiplegia with weakness sparing her face were noted; ODS was suspected. MRI revealed central pontine T2 hyperintensity, T1 hypointensity, and FLAIR hyperintensity. Treatment included gradual lowering of sodium with normal saline and free water. She was discharged to a skilled nursing facility (SNF) with sodium 138 mEq/L and upon 4-year follow-up had moderate disability and required some assistance to support activities of daily living. Our literature search yielded 23 cases (22 normonatremic; 1 where normonatremia progressed to hypernatremia). Common signs/symptoms were hyperreflexia, dysarthria, and gait disturbance. Common comorbidities were alcoholism, dialysis, and renal disease/failure. Cranial MRI confirmed all cases, frequently revealing central pontine T2 and FLAIR hyperintensity and T1 hypointensity. Our review further characterizes the diverse etiologies, clinical course, and radiographic features of ODSIN. Clinicians should consider this diagnosis when neurological symptoms occur even in the setting of normonatremia.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2024 ","pages":"6626539"},"PeriodicalIF":0.9000,"publicationDate":"2024-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11772055/pdf/","citationCount":"0","resultStr":"{\"title\":\"Osmotic Demyelination Syndrome in the Setting of Normonatremia: A Case Report and Review of the Literature.\",\"authors\":\"Rose V Zach, Jeffrey F Barletta, Victor Zach\",\"doi\":\"10.1155/crnm/6626539\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Osmotic demyelination syndrome (ODS) is a rare complication associated with rapid sodium changes, typically encountered in patients with severe hyponatremia. ODS in patients with normonatremia (ODSIN) is less recognized. We describe a patient with MRI-detected ODSIN following neurotrauma and reviewed the relevant literature. We present a 57-year-old female with subdural hematoma following ground-level fall. Her initial sodium was 140 mEq/L but over 2 days, rose 17 mEq/L, peaking at 157 mEq/L. On exam, unexplainable, unexpected left-sided hemiplegia with weakness sparing her face were noted; ODS was suspected. MRI revealed central pontine T2 hyperintensity, T1 hypointensity, and FLAIR hyperintensity. Treatment included gradual lowering of sodium with normal saline and free water. She was discharged to a skilled nursing facility (SNF) with sodium 138 mEq/L and upon 4-year follow-up had moderate disability and required some assistance to support activities of daily living. Our literature search yielded 23 cases (22 normonatremic; 1 where normonatremia progressed to hypernatremia). Common signs/symptoms were hyperreflexia, dysarthria, and gait disturbance. Common comorbidities were alcoholism, dialysis, and renal disease/failure. Cranial MRI confirmed all cases, frequently revealing central pontine T2 and FLAIR hyperintensity and T1 hypointensity. Our review further characterizes the diverse etiologies, clinical course, and radiographic features of ODSIN. Clinicians should consider this diagnosis when neurological symptoms occur even in the setting of normonatremia.</p>\",\"PeriodicalId\":9615,\"journal\":{\"name\":\"Case Reports in Neurological Medicine\",\"volume\":\"2024 \",\"pages\":\"6626539\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-11-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11772055/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Neurological Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crnm/6626539\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crnm/6626539","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Osmotic Demyelination Syndrome in the Setting of Normonatremia: A Case Report and Review of the Literature.
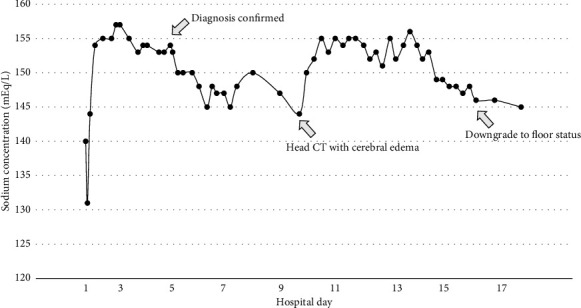
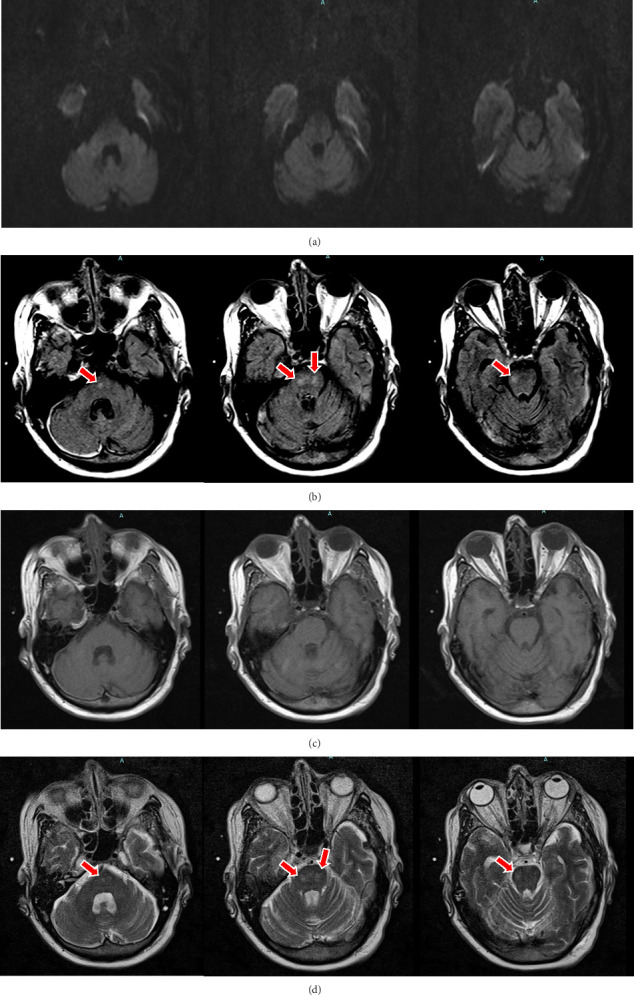
Osmotic demyelination syndrome (ODS) is a rare complication associated with rapid sodium changes, typically encountered in patients with severe hyponatremia. ODS in patients with normonatremia (ODSIN) is less recognized. We describe a patient with MRI-detected ODSIN following neurotrauma and reviewed the relevant literature. We present a 57-year-old female with subdural hematoma following ground-level fall. Her initial sodium was 140 mEq/L but over 2 days, rose 17 mEq/L, peaking at 157 mEq/L. On exam, unexplainable, unexpected left-sided hemiplegia with weakness sparing her face were noted; ODS was suspected. MRI revealed central pontine T2 hyperintensity, T1 hypointensity, and FLAIR hyperintensity. Treatment included gradual lowering of sodium with normal saline and free water. She was discharged to a skilled nursing facility (SNF) with sodium 138 mEq/L and upon 4-year follow-up had moderate disability and required some assistance to support activities of daily living. Our literature search yielded 23 cases (22 normonatremic; 1 where normonatremia progressed to hypernatremia). Common signs/symptoms were hyperreflexia, dysarthria, and gait disturbance. Common comorbidities were alcoholism, dialysis, and renal disease/failure. Cranial MRI confirmed all cases, frequently revealing central pontine T2 and FLAIR hyperintensity and T1 hypointensity. Our review further characterizes the diverse etiologies, clinical course, and radiographic features of ODSIN. Clinicians should consider this diagnosis when neurological symptoms occur even in the setting of normonatremia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


