Daseul Kim, Jae Yong Yu, Minha Kim, Gun Tak Lee, Sang Do Shin, Sung Yeon Hwang, Daun Jeong
{"title":"根据院外心脏骤停患者的转运时间间隔调整现场心肺复苏持续时间:一项全国性多中心研究。","authors":"Daseul Kim, Jae Yong Yu, Minha Kim, Gun Tak Lee, Sang Do Shin, Sung Yeon Hwang, Daun Jeong","doi":"10.1038/s41598-025-87757-3","DOIUrl":null,"url":null,"abstract":"<p><p>The optimal duration of on-scene cardiopulmonary resuscitation (CPR) for out-of-hospital cardiac arrest (OHCA) patients remains uncertain. Determining this critical time period requires outweighing the potential risks associated with intra-arrest transport while minimizing delays in accessing definitive hospital-based treatments. This study evaluated the association between on-scene CPR duration and 30-day neurologically favorable survival based on the transport time interval (TTI) in patients with OHCA. We retrospectively analyzed data from the Korean Cardiac Arrest Research Consortium registry of OHCA, comprising 65 participating hospitals in South Korea, between October 2015 and December 2021. We categorized the patients into Short-TTI (TTI < 10 min) and Long-TTI (TTI ≥ 10 min) groups. Differences in clinical features were adjusted for using propensity score matching (PSM) for TTI. The primary outcome was a 30-day neurologically favorable outcome, defined as cerebral performance category 1 or 2. Multivariable logistic regression was used to determine the variables associated with clinical outcomes. A generalized additive model based on a restricted cubic spline smooth function was utilized to infer the optimal cutoff point for on-scene CPR duration. Of the 6,345 patients, 5,844 PSM pairings were created (Short-TTI: 2,922; Long-TTI: 2,922). The primary outcome was achieved in 7.4% and 9.8% of the patients in Short-TTI and Long-TTI groups, respectively (p = 0.001). Increased on-scene CPR duration was associated with decreased neurologically favorable survival (adjusted odds ratio, 0.94; 95% confidence interval, 0.92-0.96). The optimal on-scene CPR durations in the overall PSM, Short-TTI, and Long-TTI groups were 5.1, 0, and 5.0 min, respectively. An adjusted on-scene CPR duration based on expected transport duration may be beneficial for favorable clinical outcomes in patients with OHCA.</p>","PeriodicalId":21811,"journal":{"name":"Scientific Reports","volume":"15 1","pages":"3245"},"PeriodicalIF":3.9000,"publicationDate":"2025-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11762299/pdf/","citationCount":"0","resultStr":"{\"title\":\"Adjusting on-scene CPR duration based on transport time interval in out-of-hospital cardiac arrest: a nationwide multicenter study.\",\"authors\":\"Daseul Kim, Jae Yong Yu, Minha Kim, Gun Tak Lee, Sang Do Shin, Sung Yeon Hwang, Daun Jeong\",\"doi\":\"10.1038/s41598-025-87757-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The optimal duration of on-scene cardiopulmonary resuscitation (CPR) for out-of-hospital cardiac arrest (OHCA) patients remains uncertain. Determining this critical time period requires outweighing the potential risks associated with intra-arrest transport while minimizing delays in accessing definitive hospital-based treatments. This study evaluated the association between on-scene CPR duration and 30-day neurologically favorable survival based on the transport time interval (TTI) in patients with OHCA. We retrospectively analyzed data from the Korean Cardiac Arrest Research Consortium registry of OHCA, comprising 65 participating hospitals in South Korea, between October 2015 and December 2021. We categorized the patients into Short-TTI (TTI < 10 min) and Long-TTI (TTI ≥ 10 min) groups. Differences in clinical features were adjusted for using propensity score matching (PSM) for TTI. The primary outcome was a 30-day neurologically favorable outcome, defined as cerebral performance category 1 or 2. Multivariable logistic regression was used to determine the variables associated with clinical outcomes. A generalized additive model based on a restricted cubic spline smooth function was utilized to infer the optimal cutoff point for on-scene CPR duration. Of the 6,345 patients, 5,844 PSM pairings were created (Short-TTI: 2,922; Long-TTI: 2,922). The primary outcome was achieved in 7.4% and 9.8% of the patients in Short-TTI and Long-TTI groups, respectively (p = 0.001). Increased on-scene CPR duration was associated with decreased neurologically favorable survival (adjusted odds ratio, 0.94; 95% confidence interval, 0.92-0.96). The optimal on-scene CPR durations in the overall PSM, Short-TTI, and Long-TTI groups were 5.1, 0, and 5.0 min, respectively. An adjusted on-scene CPR duration based on expected transport duration may be beneficial for favorable clinical outcomes in patients with OHCA.</p>\",\"PeriodicalId\":21811,\"journal\":{\"name\":\"Scientific Reports\",\"volume\":\"15 1\",\"pages\":\"3245\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2025-01-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11762299/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scientific Reports\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1038/s41598-025-87757-3\",\"RegionNum\":2,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scientific Reports","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1038/s41598-025-87757-3","RegionNum":2,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Adjusting on-scene CPR duration based on transport time interval in out-of-hospital cardiac arrest: a nationwide multicenter study.
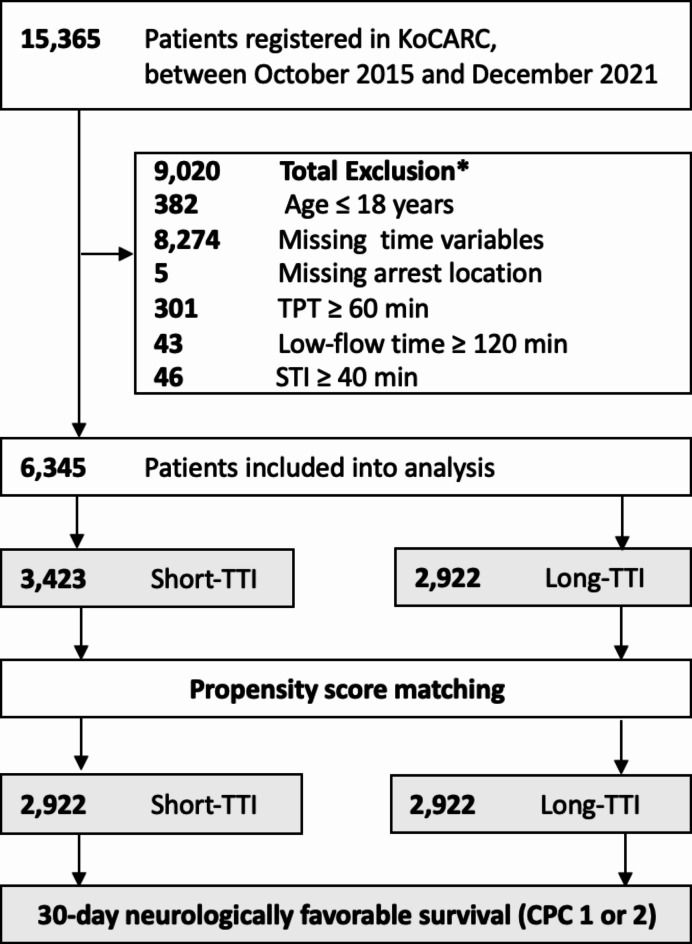
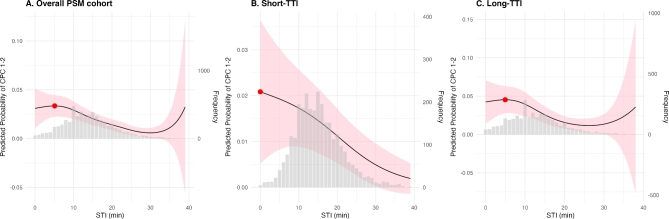
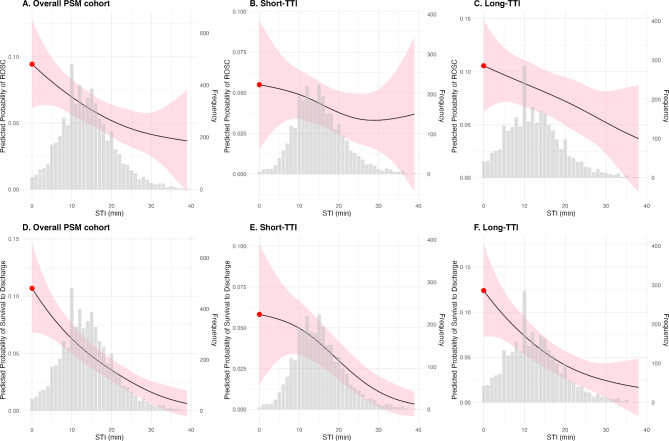
The optimal duration of on-scene cardiopulmonary resuscitation (CPR) for out-of-hospital cardiac arrest (OHCA) patients remains uncertain. Determining this critical time period requires outweighing the potential risks associated with intra-arrest transport while minimizing delays in accessing definitive hospital-based treatments. This study evaluated the association between on-scene CPR duration and 30-day neurologically favorable survival based on the transport time interval (TTI) in patients with OHCA. We retrospectively analyzed data from the Korean Cardiac Arrest Research Consortium registry of OHCA, comprising 65 participating hospitals in South Korea, between October 2015 and December 2021. We categorized the patients into Short-TTI (TTI < 10 min) and Long-TTI (TTI ≥ 10 min) groups. Differences in clinical features were adjusted for using propensity score matching (PSM) for TTI. The primary outcome was a 30-day neurologically favorable outcome, defined as cerebral performance category 1 or 2. Multivariable logistic regression was used to determine the variables associated with clinical outcomes. A generalized additive model based on a restricted cubic spline smooth function was utilized to infer the optimal cutoff point for on-scene CPR duration. Of the 6,345 patients, 5,844 PSM pairings were created (Short-TTI: 2,922; Long-TTI: 2,922). The primary outcome was achieved in 7.4% and 9.8% of the patients in Short-TTI and Long-TTI groups, respectively (p = 0.001). Increased on-scene CPR duration was associated with decreased neurologically favorable survival (adjusted odds ratio, 0.94; 95% confidence interval, 0.92-0.96). The optimal on-scene CPR durations in the overall PSM, Short-TTI, and Long-TTI groups were 5.1, 0, and 5.0 min, respectively. An adjusted on-scene CPR duration based on expected transport duration may be beneficial for favorable clinical outcomes in patients with OHCA.
期刊介绍:
We publish original research from all areas of the natural sciences, psychology, medicine and engineering. You can learn more about what we publish by browsing our specific scientific subject areas below or explore Scientific Reports by browsing all articles and collections.
Scientific Reports has a 2-year impact factor: 4.380 (2021), and is the 6th most-cited journal in the world, with more than 540,000 citations in 2020 (Clarivate Analytics, 2021).
•Engineering
Engineering covers all aspects of engineering, technology, and applied science. It plays a crucial role in the development of technologies to address some of the world''s biggest challenges, helping to save lives and improve the way we live.
•Physical sciences
Physical sciences are those academic disciplines that aim to uncover the underlying laws of nature — often written in the language of mathematics. It is a collective term for areas of study including astronomy, chemistry, materials science and physics.
•Earth and environmental sciences
Earth and environmental sciences cover all aspects of Earth and planetary science and broadly encompass solid Earth processes, surface and atmospheric dynamics, Earth system history, climate and climate change, marine and freshwater systems, and ecology. It also considers the interactions between humans and these systems.
•Biological sciences
Biological sciences encompass all the divisions of natural sciences examining various aspects of vital processes. The concept includes anatomy, physiology, cell biology, biochemistry and biophysics, and covers all organisms from microorganisms, animals to plants.
•Health sciences
The health sciences study health, disease and healthcare. This field of study aims to develop knowledge, interventions and technology for use in healthcare to improve the treatment of patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


