{"title":"探索ICU及时安全出院:机器学习预测与临床实践的比较研究。","authors":"Chao Ping Wu, Rachel Benish Shirley, Alex Milinovich, Kaiyin Liu, Eduardo Mireles-Cabodevila, Hassan Khouli, Abhijit Duggal, Anirban Bhattacharyya","doi":"10.1186/s40635-025-00717-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The discharge practices from the intensive care unit exhibit heterogeneity and the recognition of eligible patients for discharge is often delayed. Recognizing the importance of safe discharge, which aims to minimize readmission and mortality, we developed a dynamic machine-learning model. The model aims to accurately identify patients ready for discharge, offering a comparison of its effectiveness with physician decisions in terms of safety and discrepancies in discharge readiness assessment.</p><p><strong>Methods: </strong>This retrospective study uses data from patients in the medical ICU from 2015-to-2019 to develop ML models. The models were based on dynamic ICU-readily available features such as hourly vital signs, laboratory results, and interventions and were developed using various ML algorithms. The primary outcome was the hourly prediction of ICU discharge without readmission or death within 72 h post-discharge. These outcomes underwent subsequent validation within a distinct cohort from the year 2020. Additionally, the models' performance was assessed in comparison to physician judgments, with any discrepancies between the two carefully analyzed.</p><p><strong>Result: </strong>In the 2015-to-2019 cohort, the study included 17,852 unique ICU admissions. The LightGBM model outperformed other algorithms, achieving a AUROC of 0.91 (95%CI 0.9-0.91) and performance was held in the 2020 validation cohort (n = 509) with an AUROC of 0.85 (95%CI 0.84-0.85). The calibration result showed Brier score of 0.254 (95%CI 0.253-0.255). The physician agreed with the models' discharge-readiness prediction in 84.5% of patients. In patients discharged by physicians but not deemed ready by our model, the relative risk of 72-h post-ICU adverse outcomes was 2.32 (95% CI 1.1-4.9). Furthermore, the model predicted patients' readiness for discharge between 5 (IQR: 2-13.5) and 9 (IQR: 3-17) hours earlier in our selected thresholds.</p><p><strong>Conclusion: </strong>The study underscores the potential of ML models in predicting patient discharge readiness, mirroring physician behavior closely while identifying eligible patients earlier. It also highlights ML models can serve as a promising screening tool to enhance ICU discharge, presenting a pathway toward more efficient and reliable critical care decision-making.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"10"},"PeriodicalIF":2.8000,"publicationDate":"2025-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11759737/pdf/","citationCount":"0","resultStr":"{\"title\":\"Exploring timely and safe discharge from ICU: a comparative study of machine learning predictions and clinical practices.\",\"authors\":\"Chao Ping Wu, Rachel Benish Shirley, Alex Milinovich, Kaiyin Liu, Eduardo Mireles-Cabodevila, Hassan Khouli, Abhijit Duggal, Anirban Bhattacharyya\",\"doi\":\"10.1186/s40635-025-00717-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The discharge practices from the intensive care unit exhibit heterogeneity and the recognition of eligible patients for discharge is often delayed. Recognizing the importance of safe discharge, which aims to minimize readmission and mortality, we developed a dynamic machine-learning model. The model aims to accurately identify patients ready for discharge, offering a comparison of its effectiveness with physician decisions in terms of safety and discrepancies in discharge readiness assessment.</p><p><strong>Methods: </strong>This retrospective study uses data from patients in the medical ICU from 2015-to-2019 to develop ML models. The models were based on dynamic ICU-readily available features such as hourly vital signs, laboratory results, and interventions and were developed using various ML algorithms. The primary outcome was the hourly prediction of ICU discharge without readmission or death within 72 h post-discharge. These outcomes underwent subsequent validation within a distinct cohort from the year 2020. Additionally, the models' performance was assessed in comparison to physician judgments, with any discrepancies between the two carefully analyzed.</p><p><strong>Result: </strong>In the 2015-to-2019 cohort, the study included 17,852 unique ICU admissions. The LightGBM model outperformed other algorithms, achieving a AUROC of 0.91 (95%CI 0.9-0.91) and performance was held in the 2020 validation cohort (n = 509) with an AUROC of 0.85 (95%CI 0.84-0.85). The calibration result showed Brier score of 0.254 (95%CI 0.253-0.255). The physician agreed with the models' discharge-readiness prediction in 84.5% of patients. In patients discharged by physicians but not deemed ready by our model, the relative risk of 72-h post-ICU adverse outcomes was 2.32 (95% CI 1.1-4.9). Furthermore, the model predicted patients' readiness for discharge between 5 (IQR: 2-13.5) and 9 (IQR: 3-17) hours earlier in our selected thresholds.</p><p><strong>Conclusion: </strong>The study underscores the potential of ML models in predicting patient discharge readiness, mirroring physician behavior closely while identifying eligible patients earlier. It also highlights ML models can serve as a promising screening tool to enhance ICU discharge, presenting a pathway toward more efficient and reliable critical care decision-making.</p>\",\"PeriodicalId\":13750,\"journal\":{\"name\":\"Intensive Care Medicine Experimental\",\"volume\":\"13 1\",\"pages\":\"10\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-01-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11759737/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Intensive Care Medicine Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40635-025-00717-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00717-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Exploring timely and safe discharge from ICU: a comparative study of machine learning predictions and clinical practices.
Background: The discharge practices from the intensive care unit exhibit heterogeneity and the recognition of eligible patients for discharge is often delayed. Recognizing the importance of safe discharge, which aims to minimize readmission and mortality, we developed a dynamic machine-learning model. The model aims to accurately identify patients ready for discharge, offering a comparison of its effectiveness with physician decisions in terms of safety and discrepancies in discharge readiness assessment.
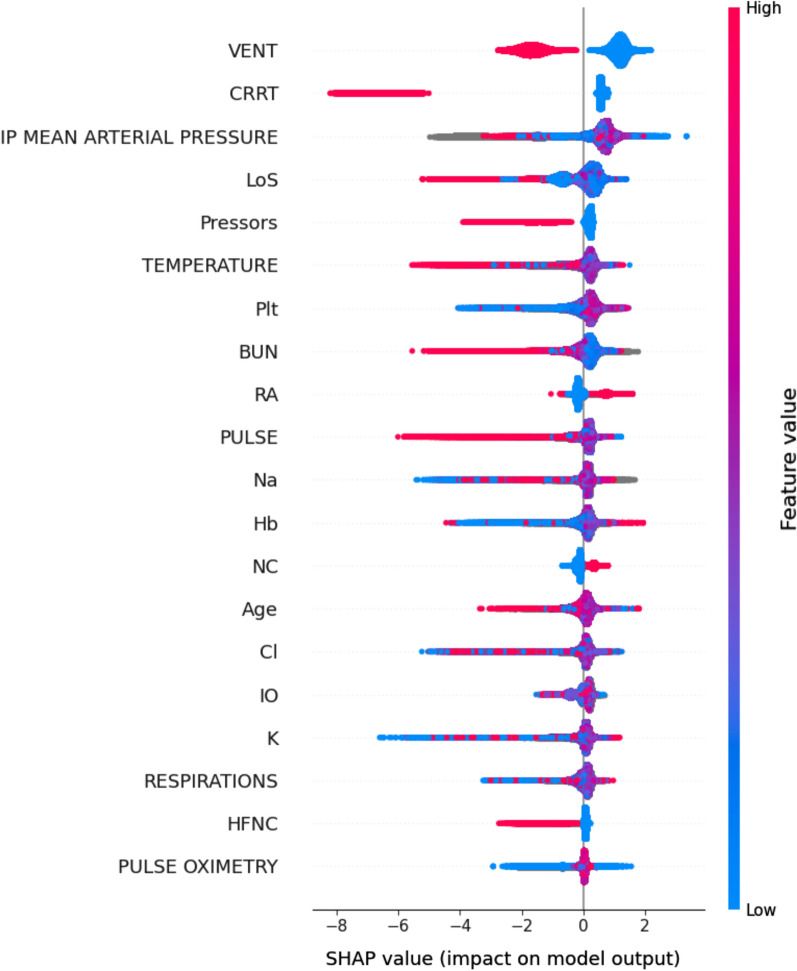
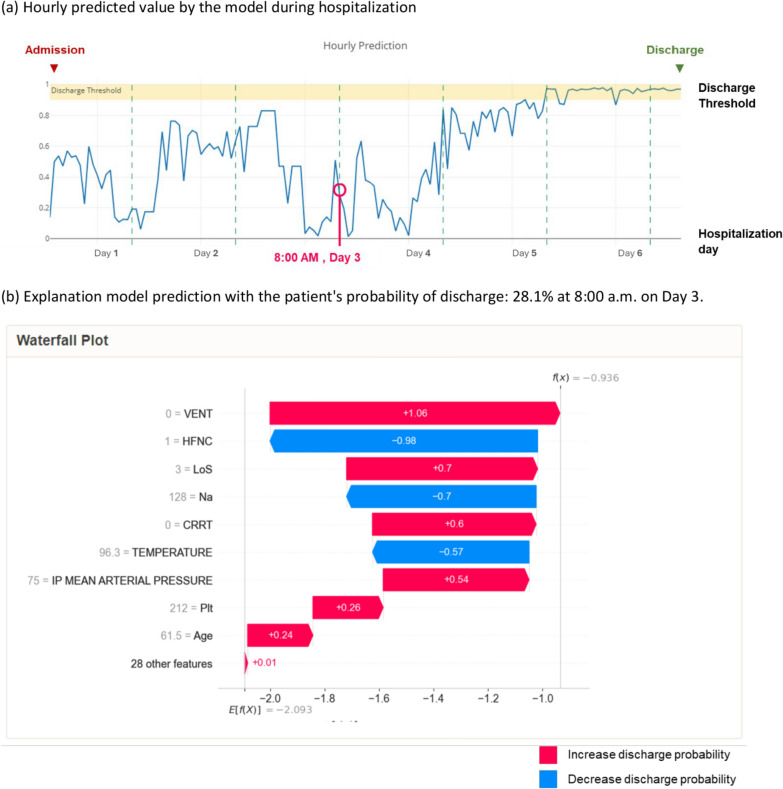
Methods: This retrospective study uses data from patients in the medical ICU from 2015-to-2019 to develop ML models. The models were based on dynamic ICU-readily available features such as hourly vital signs, laboratory results, and interventions and were developed using various ML algorithms. The primary outcome was the hourly prediction of ICU discharge without readmission or death within 72 h post-discharge. These outcomes underwent subsequent validation within a distinct cohort from the year 2020. Additionally, the models' performance was assessed in comparison to physician judgments, with any discrepancies between the two carefully analyzed.
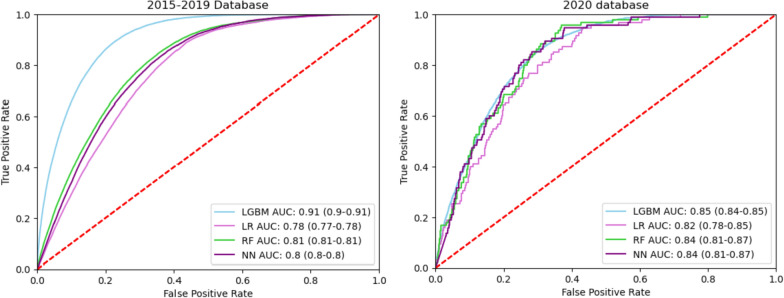
Result: In the 2015-to-2019 cohort, the study included 17,852 unique ICU admissions. The LightGBM model outperformed other algorithms, achieving a AUROC of 0.91 (95%CI 0.9-0.91) and performance was held in the 2020 validation cohort (n = 509) with an AUROC of 0.85 (95%CI 0.84-0.85). The calibration result showed Brier score of 0.254 (95%CI 0.253-0.255). The physician agreed with the models' discharge-readiness prediction in 84.5% of patients. In patients discharged by physicians but not deemed ready by our model, the relative risk of 72-h post-ICU adverse outcomes was 2.32 (95% CI 1.1-4.9). Furthermore, the model predicted patients' readiness for discharge between 5 (IQR: 2-13.5) and 9 (IQR: 3-17) hours earlier in our selected thresholds.
Conclusion: The study underscores the potential of ML models in predicting patient discharge readiness, mirroring physician behavior closely while identifying eligible patients earlier. It also highlights ML models can serve as a promising screening tool to enhance ICU discharge, presenting a pathway toward more efficient and reliable critical care decision-making.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


