Niwen Kong, Patrick Chang, Ira A Shulman, Ubayd Haq, Maziar Amini, Denis Nguyen, Farhaad Khan, Rachan Narala, Nisha Sharma, Daniel Wang, Tiana Thompson, Jonathan Sadik, Cameron Breze, David C Whitcomb, James L Buxbaum
{"title":"机器学习引导的急性胰腺炎液体复苏改善预后","authors":"Niwen Kong, Patrick Chang, Ira A Shulman, Ubayd Haq, Maziar Amini, Denis Nguyen, Farhaad Khan, Rachan Narala, Nisha Sharma, Daniel Wang, Tiana Thompson, Jonathan Sadik, Cameron Breze, David C Whitcomb, James L Buxbaum","doi":"10.14309/ctg.0000000000000825","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Ariel Dynamic Acute Pancreatitis Tracker (ADAPT) is an artificial intelligence tool using mathematical algorithms to predict severity and manage fluid resuscitation needs based on the physiologic parameters of individual patients. Our aim was to assess whether adherence to ADAPT fluid recommendations vs standard management impacted clinical outcomes in a large prospective cohort.</p><p><strong>Methods: </strong>We analyzed patients consecutively admitted to the Los Angeles General Medical Center between June 2015 and November 2022 whose course was richly characterized by capturing more than 100 clinical variables. We inputted these data into the ADAPT system to generate resuscitation fluid recommendations and compared with the actual fluid resuscitation within the first 24 hours from presentation. The primary outcome was the difference in organ failure in those who were over-resuscitated (>500 mL) vs adequately resuscitated (within 500 mL) with respect to the ADAPT fluid recommendation. Additional outcomes included intensive care unit admission, systemic inflammatory response syndrome (SIRS) at 48 hours, local complications, and pancreatitis severity.</p><p><strong>Results: </strong>Among the 1,083 patients evaluated using ADAPT, 700 were over-resuscitated, 196 were adequately resuscitated, and 187 were under-resuscitated. Adjusting for pancreatitis etiology, gender, and SIRS at admission, over-resuscitation was associated with increased respiratory failure (odd ratio [OR] 2.73, 95% confidence interval [CI] 1.06-7.03) as well as intensive care unit admission (OR 2.40, 1.41-4.11), more than 48 hours of hospital length of stay (OR 1.87, 95% CI 1.19-2.94), SIRS at 48 hours (OR 1.73, 95% CI 1.08-2.77), and local pancreatitis complications (OR 2.93, 95% CI 1.23-6.96).</p><p><strong>Discussion: </strong>Adherence to ADAPT fluid recommendations reduces respiratory failure and other adverse outcomes compared with conventional fluid resuscitation strategies for acute pancreatitis. This validation study demonstrates the potential role of dynamic machine learning tools in acute pancreatitis management.</p>","PeriodicalId":10278,"journal":{"name":"Clinical and Translational Gastroenterology","volume":" ","pages":"e00825"},"PeriodicalIF":3.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020695/pdf/","citationCount":"0","resultStr":"{\"title\":\"Machine Learning-Guided Fluid Resuscitation for Acute Pancreatitis Improves Outcomes.\",\"authors\":\"Niwen Kong, Patrick Chang, Ira A Shulman, Ubayd Haq, Maziar Amini, Denis Nguyen, Farhaad Khan, Rachan Narala, Nisha Sharma, Daniel Wang, Tiana Thompson, Jonathan Sadik, Cameron Breze, David C Whitcomb, James L Buxbaum\",\"doi\":\"10.14309/ctg.0000000000000825\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Ariel Dynamic Acute Pancreatitis Tracker (ADAPT) is an artificial intelligence tool using mathematical algorithms to predict severity and manage fluid resuscitation needs based on the physiologic parameters of individual patients. Our aim was to assess whether adherence to ADAPT fluid recommendations vs standard management impacted clinical outcomes in a large prospective cohort.</p><p><strong>Methods: </strong>We analyzed patients consecutively admitted to the Los Angeles General Medical Center between June 2015 and November 2022 whose course was richly characterized by capturing more than 100 clinical variables. We inputted these data into the ADAPT system to generate resuscitation fluid recommendations and compared with the actual fluid resuscitation within the first 24 hours from presentation. The primary outcome was the difference in organ failure in those who were over-resuscitated (>500 mL) vs adequately resuscitated (within 500 mL) with respect to the ADAPT fluid recommendation. Additional outcomes included intensive care unit admission, systemic inflammatory response syndrome (SIRS) at 48 hours, local complications, and pancreatitis severity.</p><p><strong>Results: </strong>Among the 1,083 patients evaluated using ADAPT, 700 were over-resuscitated, 196 were adequately resuscitated, and 187 were under-resuscitated. Adjusting for pancreatitis etiology, gender, and SIRS at admission, over-resuscitation was associated with increased respiratory failure (odd ratio [OR] 2.73, 95% confidence interval [CI] 1.06-7.03) as well as intensive care unit admission (OR 2.40, 1.41-4.11), more than 48 hours of hospital length of stay (OR 1.87, 95% CI 1.19-2.94), SIRS at 48 hours (OR 1.73, 95% CI 1.08-2.77), and local pancreatitis complications (OR 2.93, 95% CI 1.23-6.96).</p><p><strong>Discussion: </strong>Adherence to ADAPT fluid recommendations reduces respiratory failure and other adverse outcomes compared with conventional fluid resuscitation strategies for acute pancreatitis. This validation study demonstrates the potential role of dynamic machine learning tools in acute pancreatitis management.</p>\",\"PeriodicalId\":10278,\"journal\":{\"name\":\"Clinical and Translational Gastroenterology\",\"volume\":\" \",\"pages\":\"e00825\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020695/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14309/ctg.0000000000000825\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14309/ctg.0000000000000825","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Machine Learning-Guided Fluid Resuscitation for Acute Pancreatitis Improves Outcomes.
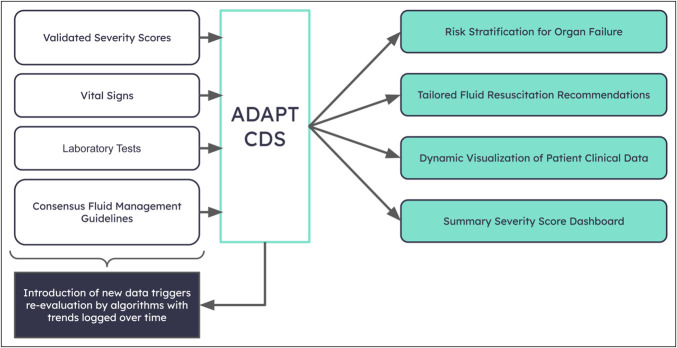
Introduction: Ariel Dynamic Acute Pancreatitis Tracker (ADAPT) is an artificial intelligence tool using mathematical algorithms to predict severity and manage fluid resuscitation needs based on the physiologic parameters of individual patients. Our aim was to assess whether adherence to ADAPT fluid recommendations vs standard management impacted clinical outcomes in a large prospective cohort.
Methods: We analyzed patients consecutively admitted to the Los Angeles General Medical Center between June 2015 and November 2022 whose course was richly characterized by capturing more than 100 clinical variables. We inputted these data into the ADAPT system to generate resuscitation fluid recommendations and compared with the actual fluid resuscitation within the first 24 hours from presentation. The primary outcome was the difference in organ failure in those who were over-resuscitated (>500 mL) vs adequately resuscitated (within 500 mL) with respect to the ADAPT fluid recommendation. Additional outcomes included intensive care unit admission, systemic inflammatory response syndrome (SIRS) at 48 hours, local complications, and pancreatitis severity.
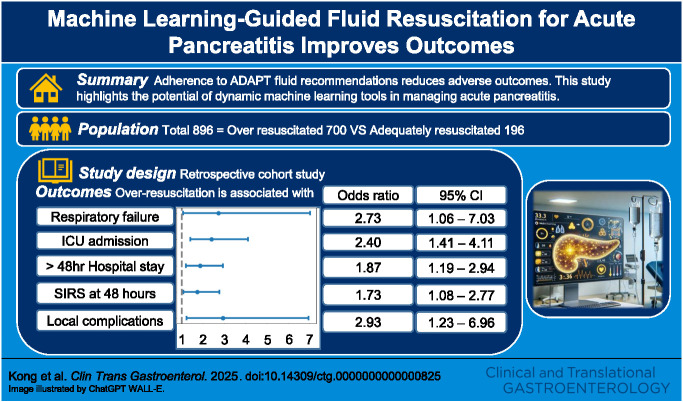
Results: Among the 1,083 patients evaluated using ADAPT, 700 were over-resuscitated, 196 were adequately resuscitated, and 187 were under-resuscitated. Adjusting for pancreatitis etiology, gender, and SIRS at admission, over-resuscitation was associated with increased respiratory failure (odd ratio [OR] 2.73, 95% confidence interval [CI] 1.06-7.03) as well as intensive care unit admission (OR 2.40, 1.41-4.11), more than 48 hours of hospital length of stay (OR 1.87, 95% CI 1.19-2.94), SIRS at 48 hours (OR 1.73, 95% CI 1.08-2.77), and local pancreatitis complications (OR 2.93, 95% CI 1.23-6.96).
Discussion: Adherence to ADAPT fluid recommendations reduces respiratory failure and other adverse outcomes compared with conventional fluid resuscitation strategies for acute pancreatitis. This validation study demonstrates the potential role of dynamic machine learning tools in acute pancreatitis management.
期刊介绍:
Clinical and Translational Gastroenterology (CTG), published on behalf of the American College of Gastroenterology (ACG), is a peer-reviewed open access online journal dedicated to innovative clinical work in the field of gastroenterology and hepatology. CTG hopes to fulfill an unmet need for clinicians and scientists by welcoming novel cohort studies, early-phase clinical trials, qualitative and quantitative epidemiologic research, hypothesis-generating research, studies of novel mechanisms and methodologies including public health interventions, and integration of approaches across organs and disciplines. CTG also welcomes hypothesis-generating small studies, methods papers, and translational research with clear applications to human physiology or disease.
Colon and small bowel
Endoscopy and novel diagnostics
Esophagus
Functional GI disorders
Immunology of the GI tract
Microbiology of the GI tract
Inflammatory bowel disease
Pancreas and biliary tract
Liver
Pathology
Pediatrics
Preventative medicine
Nutrition/obesity
Stomach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


