Mbali Precious Nkosi, Keegan John Hoog, Michelle Lowe
{"title":"南非乙氏肺囊虫肺炎(2018-2022)。","authors":"Mbali Precious Nkosi, Keegan John Hoog, Michelle Lowe","doi":"10.1093/mmy/myaf001","DOIUrl":null,"url":null,"abstract":"<p><p>Pneumocystis jirovecii causes P. jirovecii pneumonia (PJP)-a leading opportunistic infection among persons with advanced human immunodeficiency virus. Furthermore, individuals with underlying conditions such as cancer and transplant recipients are susceptible to PJP. Most data on PJP come from other countries, with limited knowledge about its prevalence in Africa. The aim was to describe changes in the proportion of positive PJP tests in South Africa from 2018 to 2022. A 5-year retrospective study was conducted on patients with suspected P. jirovecii, detected by polymerase chain reaction. Data were obtained from the National Health Laboratory Service, where laboratory diagnostics were done as part of routine patient care. Mann-Whitney test and Χ2 tests were used to compare the age, sex, and wards with both the negative and positive results of PJP. From 2018 to 2022, a total of 8110 patients' results were retrieved, and 8059 met the inclusion criteria. The positive test proportions of PJP in South Africa were 32.66%, 29.93%, 34.02%, 24.98%, and 25.78%, respectively. The median age was 35 years, with interquartile range of 24-43 years (P = .002). Female patients had a higher positive test proportion than males (59.39% vs. 38.74%, P < .001). The proportion of positive PJP tests was higher in general wards (48.54%) and intensive care units (18.99%) (P = .012). The epidemiology of PJP in South Africa is similar to that of other countries in some respects but is influenced by unique factors specific to the country. These findings are crucial for public health planning, emphasising the need for targeted PJP prevention strategies considering sex- and age-specific vulnerabilities in South Africa.</p>","PeriodicalId":18586,"journal":{"name":"Medical mycology","volume":" ","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11761960/pdf/","citationCount":"0","resultStr":"{\"title\":\"Insights into Pneumocystis jirovecii pneumonia in South Africa (2018-2022).\",\"authors\":\"Mbali Precious Nkosi, Keegan John Hoog, Michelle Lowe\",\"doi\":\"10.1093/mmy/myaf001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Pneumocystis jirovecii causes P. jirovecii pneumonia (PJP)-a leading opportunistic infection among persons with advanced human immunodeficiency virus. Furthermore, individuals with underlying conditions such as cancer and transplant recipients are susceptible to PJP. Most data on PJP come from other countries, with limited knowledge about its prevalence in Africa. The aim was to describe changes in the proportion of positive PJP tests in South Africa from 2018 to 2022. A 5-year retrospective study was conducted on patients with suspected P. jirovecii, detected by polymerase chain reaction. Data were obtained from the National Health Laboratory Service, where laboratory diagnostics were done as part of routine patient care. Mann-Whitney test and Χ2 tests were used to compare the age, sex, and wards with both the negative and positive results of PJP. From 2018 to 2022, a total of 8110 patients' results were retrieved, and 8059 met the inclusion criteria. The positive test proportions of PJP in South Africa were 32.66%, 29.93%, 34.02%, 24.98%, and 25.78%, respectively. The median age was 35 years, with interquartile range of 24-43 years (P = .002). Female patients had a higher positive test proportion than males (59.39% vs. 38.74%, P < .001). The proportion of positive PJP tests was higher in general wards (48.54%) and intensive care units (18.99%) (P = .012). The epidemiology of PJP in South Africa is similar to that of other countries in some respects but is influenced by unique factors specific to the country. These findings are crucial for public health planning, emphasising the need for targeted PJP prevention strategies considering sex- and age-specific vulnerabilities in South Africa.</p>\",\"PeriodicalId\":18586,\"journal\":{\"name\":\"Medical mycology\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-01-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11761960/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical mycology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/mmy/myaf001\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical mycology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/mmy/myaf001","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
摘要
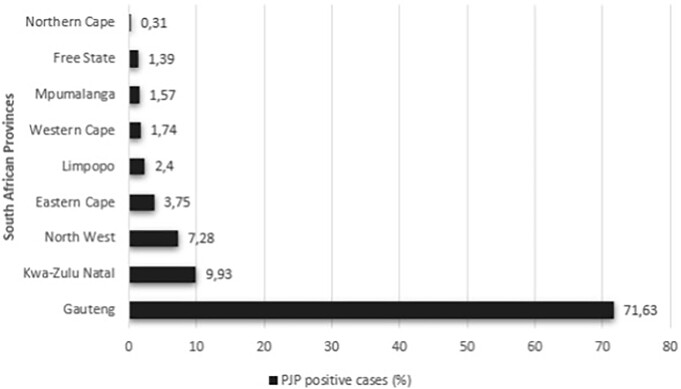
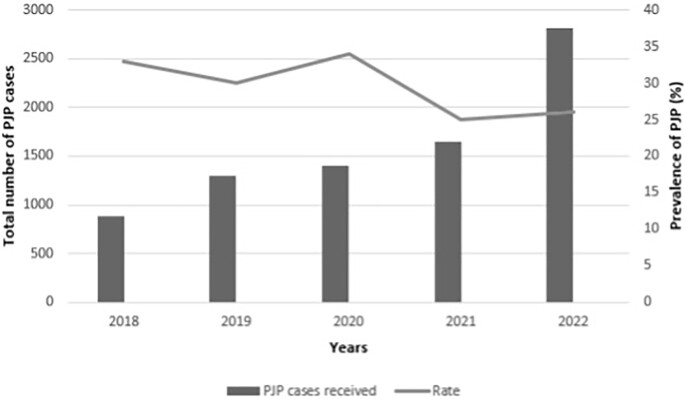
耶氏肺囊虫(耶氏肺囊虫)引起耶氏肺囊虫肺炎(PJP),这是晚期人类免疫缺陷病毒(HIV)感染者中主要的机会性感染。此外,患有癌症和移植受者等潜在疾病的个体易患PJP。关于PJP的大多数数据来自其他国家,对其在非洲的流行情况了解有限。目的是描述2018年至2022年南非PJP阳性检测比例的变化。采用聚合酶链反应(PCR)对疑似感染耶氏疟原虫的患者进行了为期五年的回顾性研究。数据来自国家卫生实验室服务(NHLS),实验室诊断是作为常规患者护理的一部分进行的。采用Mann-Whitney检验和卡方检验比较PJP阴性和阳性结果与年龄、性别、病房的关系。2018 - 2022年共检索8110例患者的结果,其中8059例符合纳入标准。PJP在SA中的阳性检出率分别为32.66%、29.93%、34.02%、24.98%和25.78%。年龄中位数为35岁,四分位数间距(IQR)为24 ~ 43岁(p = 0.002)。女性患者的阳性检测比例高于男性(59.39% vs 38.74%, p
Insights into Pneumocystis jirovecii pneumonia in South Africa (2018-2022).
Pneumocystis jirovecii causes P. jirovecii pneumonia (PJP)-a leading opportunistic infection among persons with advanced human immunodeficiency virus. Furthermore, individuals with underlying conditions such as cancer and transplant recipients are susceptible to PJP. Most data on PJP come from other countries, with limited knowledge about its prevalence in Africa. The aim was to describe changes in the proportion of positive PJP tests in South Africa from 2018 to 2022. A 5-year retrospective study was conducted on patients with suspected P. jirovecii, detected by polymerase chain reaction. Data were obtained from the National Health Laboratory Service, where laboratory diagnostics were done as part of routine patient care. Mann-Whitney test and Χ2 tests were used to compare the age, sex, and wards with both the negative and positive results of PJP. From 2018 to 2022, a total of 8110 patients' results were retrieved, and 8059 met the inclusion criteria. The positive test proportions of PJP in South Africa were 32.66%, 29.93%, 34.02%, 24.98%, and 25.78%, respectively. The median age was 35 years, with interquartile range of 24-43 years (P = .002). Female patients had a higher positive test proportion than males (59.39% vs. 38.74%, P < .001). The proportion of positive PJP tests was higher in general wards (48.54%) and intensive care units (18.99%) (P = .012). The epidemiology of PJP in South Africa is similar to that of other countries in some respects but is influenced by unique factors specific to the country. These findings are crucial for public health planning, emphasising the need for targeted PJP prevention strategies considering sex- and age-specific vulnerabilities in South Africa.
期刊介绍:
Medical Mycology is a peer-reviewed international journal that focuses on original and innovative basic and applied studies, as well as learned reviews on all aspects of medical, veterinary and environmental mycology as related to disease. The objective is to present the highest quality scientific reports from throughout the world on divergent topics. These topics include the phylogeny of fungal pathogens, epidemiology and public health mycology themes, new approaches in the diagnosis and treatment of mycoses including clinical trials and guidelines, pharmacology and antifungal susceptibilities, changes in taxonomy, description of new or unusual fungi associated with human or animal disease, immunology of fungal infections, vaccinology for prevention of fungal infections, pathogenesis and virulence, and the molecular biology of pathogenic fungi in vitro and in vivo, including genomics, transcriptomics, metabolomics, and proteomics. Case reports are no longer accepted. In addition, studies of natural products showing inhibitory activity against pathogenic fungi are not accepted without chemical characterization and identification of the compounds responsible for the inhibitory activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


