Ivan Y Luu, Alexander T Hong, Ashton Lee, Juan C Arias, Chia-Ding Shih, David G Armstrong, Tze-Woei Tan
{"title":"改善糖尿病足溃疡结局的医疗补助受益人与足部护理途径。","authors":"Ivan Y Luu, Alexander T Hong, Ashton Lee, Juan C Arias, Chia-Ding Shih, David G Armstrong, Tze-Woei Tan","doi":"10.3390/diabetology5050036","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study aims to examine the association between state Medicaid coverage of podiatry services and the outcomes of beneficiaries with new diabetic foot ulcers (DFUs).</p><p><strong>Methods: </strong>Medicaid beneficiaries who developed a DFU between 2010 and 2015 were identified using the PearlDiver claims database. The states were categorized into covered states (CS) and non-covered states (NCS) based on podiatric coverage during the study period. The outcomes included major amputation, minor amputation, and hospitalization due to foot infection within 12 months of index diagnosis. Logistic regression was used to assess the association of state coverage type and outcomes, controlling for age, sex, and the Charlson Comorbidity Index (CCI).</p><p><strong>Results: </strong>Our study included 16,905 Medicaid beneficiaries who developed new DFUs: 14,748 in CS and 2157 in NCS. The overall major amputation rate was 2.6%. The risk of major amputation was 48% lower among Medicaid beneficiaries in CS (OR 0.52, 95% CI 0.31-0.90) than in NCS. The Medicaid beneficiaries in CS had a 24% lower risk of hospitalization for foot infection (OR 0.76, 95% CI 0.67-0.85) but had a 58% higher risk of minor amputation (OR 1.58, 95% CI 1.22-2.07) than in NCS.</p><p><strong>Conclusions: </strong>Medicaid coverage of podiatry services might be associated with lower rates of major amputation and reduced risk of hospitalization for foot infection.</p>","PeriodicalId":72798,"journal":{"name":"Diabetology","volume":"5 5","pages":"491-500"},"PeriodicalIF":2.2000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11706342/pdf/","citationCount":"0","resultStr":"{\"title\":\"Improved Diabetic Foot Ulcer Outcomes in Medicaid Beneficiaries with Podiatric Care Access.\",\"authors\":\"Ivan Y Luu, Alexander T Hong, Ashton Lee, Juan C Arias, Chia-Ding Shih, David G Armstrong, Tze-Woei Tan\",\"doi\":\"10.3390/diabetology5050036\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>This study aims to examine the association between state Medicaid coverage of podiatry services and the outcomes of beneficiaries with new diabetic foot ulcers (DFUs).</p><p><strong>Methods: </strong>Medicaid beneficiaries who developed a DFU between 2010 and 2015 were identified using the PearlDiver claims database. The states were categorized into covered states (CS) and non-covered states (NCS) based on podiatric coverage during the study period. The outcomes included major amputation, minor amputation, and hospitalization due to foot infection within 12 months of index diagnosis. Logistic regression was used to assess the association of state coverage type and outcomes, controlling for age, sex, and the Charlson Comorbidity Index (CCI).</p><p><strong>Results: </strong>Our study included 16,905 Medicaid beneficiaries who developed new DFUs: 14,748 in CS and 2157 in NCS. The overall major amputation rate was 2.6%. The risk of major amputation was 48% lower among Medicaid beneficiaries in CS (OR 0.52, 95% CI 0.31-0.90) than in NCS. The Medicaid beneficiaries in CS had a 24% lower risk of hospitalization for foot infection (OR 0.76, 95% CI 0.67-0.85) but had a 58% higher risk of minor amputation (OR 1.58, 95% CI 1.22-2.07) than in NCS.</p><p><strong>Conclusions: </strong>Medicaid coverage of podiatry services might be associated with lower rates of major amputation and reduced risk of hospitalization for foot infection.</p>\",\"PeriodicalId\":72798,\"journal\":{\"name\":\"Diabetology\",\"volume\":\"5 5\",\"pages\":\"491-500\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11706342/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/diabetology5050036\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/diabetology5050036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
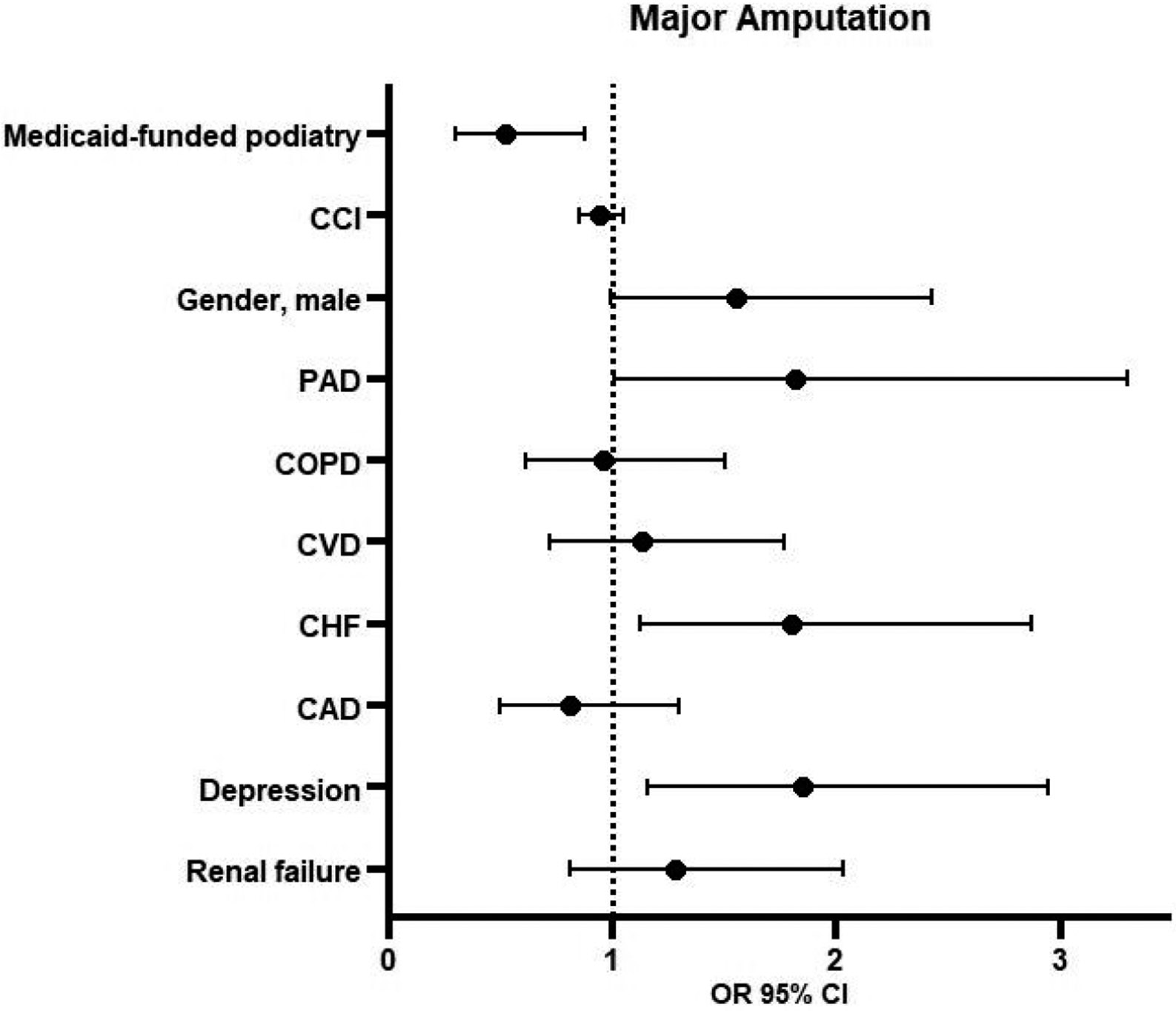
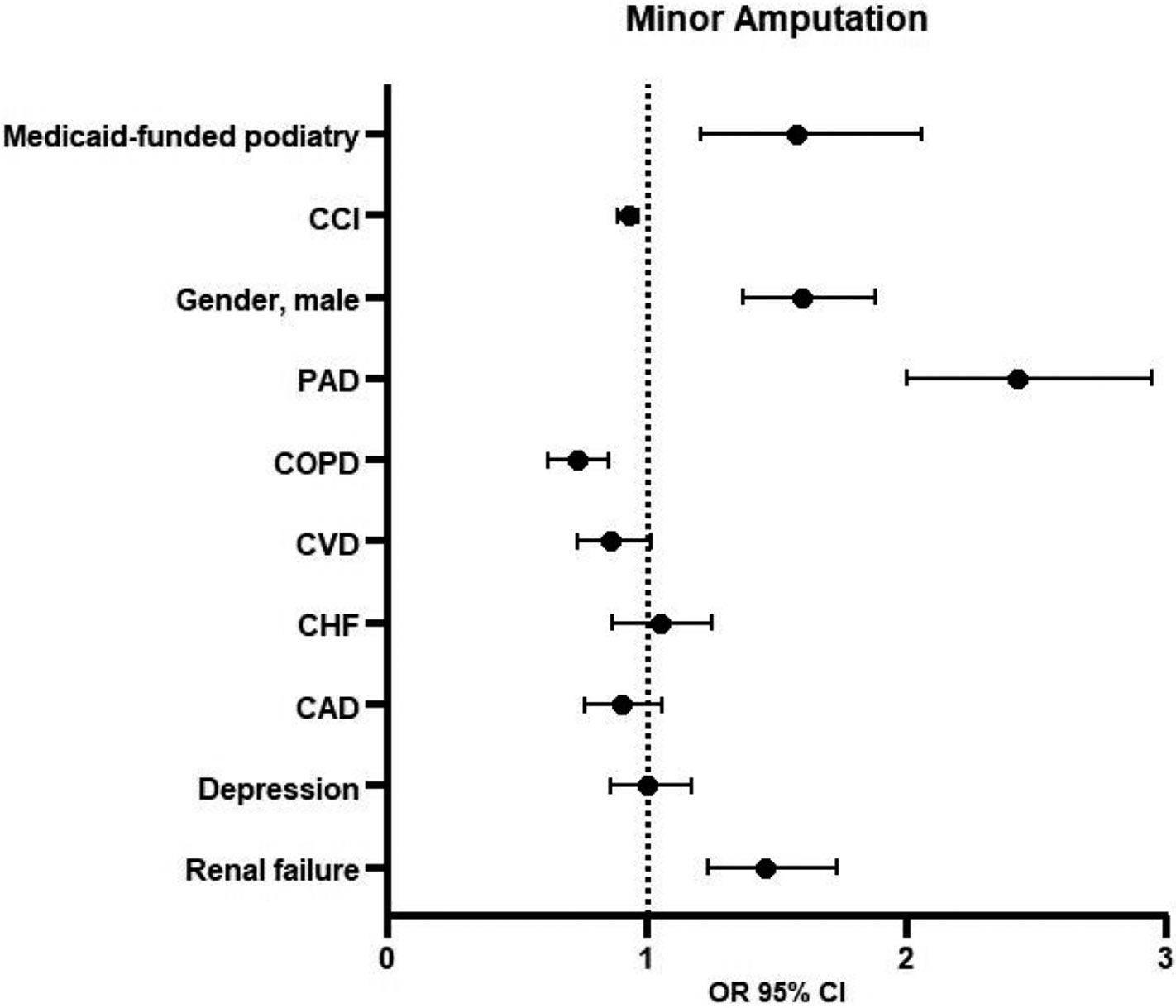
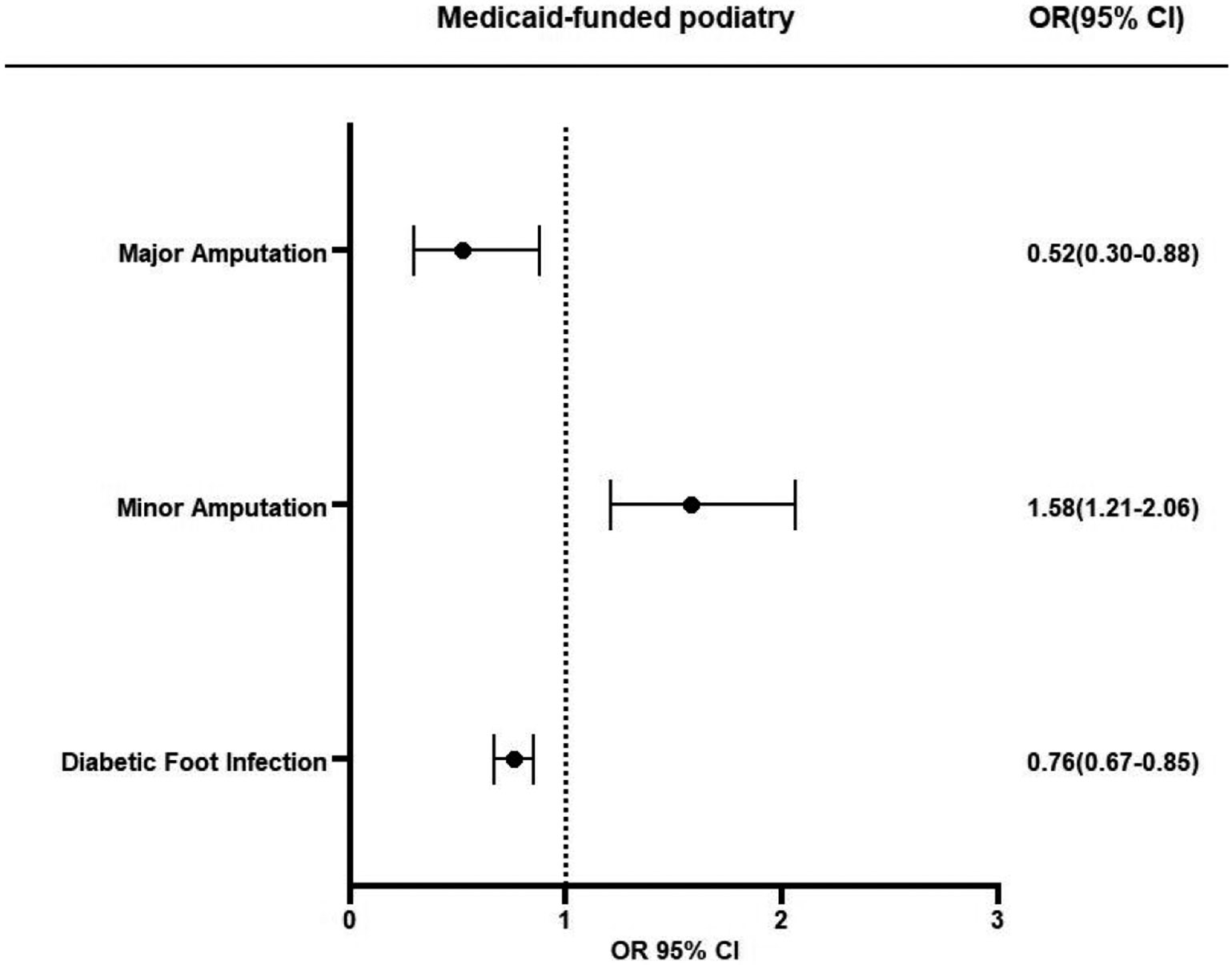
目的:本研究旨在研究国家医疗补助足部服务覆盖率与新发糖尿病足溃疡(DFUs)受益人结局之间的关系。方法:2010年至2015年间发生DFU的医疗补助受益人使用PearlDiver索赔数据库进行识别。根据研究期间的足病覆盖率,将这些州分为覆盖州(CS)和非覆盖州(NCS)。结果包括主要截肢、轻微截肢和在指标诊断后12个月内因足部感染住院。在控制年龄、性别和Charlson合并症指数(CCI)的情况下,使用逻辑回归来评估州覆盖类型和结果的关联。结果:我们的研究包括16,905名出现新的DFUs的医疗补助受益人:CS为14,748人,NCS为2157人。总体主要截肢率为2.6%。CS患者的主要截肢风险比NCS患者低48% (OR 0.52, 95% CI 0.31-0.90)。CS的医疗补助受益人因足部感染住院的风险比NCS低24% (OR 0.76, 95% CI 0.67-0.85),但小截肢的风险比NCS高58% (OR 1.58, 95% CI 1.22-2.07)。结论:医疗补助覆盖足部服务可能与较低的截肢率和足部感染住院风险有关。
Improved Diabetic Foot Ulcer Outcomes in Medicaid Beneficiaries with Podiatric Care Access.
Objectives: This study aims to examine the association between state Medicaid coverage of podiatry services and the outcomes of beneficiaries with new diabetic foot ulcers (DFUs).
Methods: Medicaid beneficiaries who developed a DFU between 2010 and 2015 were identified using the PearlDiver claims database. The states were categorized into covered states (CS) and non-covered states (NCS) based on podiatric coverage during the study period. The outcomes included major amputation, minor amputation, and hospitalization due to foot infection within 12 months of index diagnosis. Logistic regression was used to assess the association of state coverage type and outcomes, controlling for age, sex, and the Charlson Comorbidity Index (CCI).
Results: Our study included 16,905 Medicaid beneficiaries who developed new DFUs: 14,748 in CS and 2157 in NCS. The overall major amputation rate was 2.6%. The risk of major amputation was 48% lower among Medicaid beneficiaries in CS (OR 0.52, 95% CI 0.31-0.90) than in NCS. The Medicaid beneficiaries in CS had a 24% lower risk of hospitalization for foot infection (OR 0.76, 95% CI 0.67-0.85) but had a 58% higher risk of minor amputation (OR 1.58, 95% CI 1.22-2.07) than in NCS.
Conclusions: Medicaid coverage of podiatry services might be associated with lower rates of major amputation and reduced risk of hospitalization for foot infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


