Angiza Shahim, Cecilia Linde, Gianluigi Savarese, Ulf Dahlström, Lars H. Lund, Camilla Hage
{"title":"根据心力衰竭持续时间降低射血分数的心力衰竭指南推荐疗法的实施:来自瑞典心力衰竭(SwedeHF)登记处的55581例患者的分析","authors":"Angiza Shahim, Cecilia Linde, Gianluigi Savarese, Ulf Dahlström, Lars H. Lund, Camilla Hage","doi":"10.1002/ejhf.3565","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>Guidelines recommend immediate initiation of all four class I guideline-directed medical therapies, renin–angiotensin system inhibitors (RASI) or angiotensin receptor–neprilysin inhibitors (ARNI), beta-blockers, mineralocorticoid receptor antagonists (MRA) and sodium–glucose cotransporter 2 inhibitors (SGLT2i) following the diagnosis of heart failure (HF) with reduced ejection fraction (HFrEF). The extent to which this occurs in new-onset HFrEF is unclear. We assessed guideline-recommended therapies during the first year following a HFrEF diagnosis.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>The Swedish HF Registry was linked to additional national registries. In patients with HFrEF (ejection fraction <40%), clinical characteristics and HF treatment from when they were available and recommended in guidelines were assessed according to time from HF diagnosis (<3, 3 to <6, 6–12 and >12 months). Of 55 581 patients with HFrEF enrolled between 2000 and 2021, 54%, 5.8%, 4.8% and 36% had an HF duration of <3, 3 to <6, 6–12 and >12 months, respectively. Patients with shorter HF duration were younger, had lower New York Heart Association class and had fewer cardiovascular comorbidities. Within 3 months, 3 to <6 months, 6–12 months and >12 months from HF diagnosis, 93%, 92%, 90% and 89% were on RASI or ARNI, 9.8%, 17%, 19% and 22% on ARNI alone, 35%, 43%, 44% and 46% on MRA, 92%, 92%, 92% and 91% on beta-blockers, and 26%, 30%, 19% and 28% on SGLT2i, respectively. Additionally, 18% received cardiac resynchronization therapy/implantable cardioverter-defibrillator >12 months after diagnosis.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Most patients received RASI and beta-blockers in the first months following HFrEF diagnosis. Use of ARNI, MRA and SGLT2i was limited, both in the early and later time periods. Our findings suggest that strategies to improve guideline-directed use of HFrEF therapies remain urgently needed.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"27 3","pages":"421-431"},"PeriodicalIF":16.9000,"publicationDate":"2025-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3565","citationCount":"0","resultStr":"{\"title\":\"Implementation of guideline-recommended therapies in heart failure with reduced ejection fraction according to heart failure duration: An analysis of 55 581 patients from the Swedish Heart Failure (SwedeHF) Registry\",\"authors\":\"Angiza Shahim, Cecilia Linde, Gianluigi Savarese, Ulf Dahlström, Lars H. Lund, Camilla Hage\",\"doi\":\"10.1002/ejhf.3565\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Guidelines recommend immediate initiation of all four class I guideline-directed medical therapies, renin–angiotensin system inhibitors (RASI) or angiotensin receptor–neprilysin inhibitors (ARNI), beta-blockers, mineralocorticoid receptor antagonists (MRA) and sodium–glucose cotransporter 2 inhibitors (SGLT2i) following the diagnosis of heart failure (HF) with reduced ejection fraction (HFrEF). The extent to which this occurs in new-onset HFrEF is unclear. We assessed guideline-recommended therapies during the first year following a HFrEF diagnosis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>The Swedish HF Registry was linked to additional national registries. In patients with HFrEF (ejection fraction <40%), clinical characteristics and HF treatment from when they were available and recommended in guidelines were assessed according to time from HF diagnosis (<3, 3 to <6, 6–12 and >12 months). Of 55 581 patients with HFrEF enrolled between 2000 and 2021, 54%, 5.8%, 4.8% and 36% had an HF duration of <3, 3 to <6, 6–12 and >12 months, respectively. Patients with shorter HF duration were younger, had lower New York Heart Association class and had fewer cardiovascular comorbidities. Within 3 months, 3 to <6 months, 6–12 months and >12 months from HF diagnosis, 93%, 92%, 90% and 89% were on RASI or ARNI, 9.8%, 17%, 19% and 22% on ARNI alone, 35%, 43%, 44% and 46% on MRA, 92%, 92%, 92% and 91% on beta-blockers, and 26%, 30%, 19% and 28% on SGLT2i, respectively. Additionally, 18% received cardiac resynchronization therapy/implantable cardioverter-defibrillator >12 months after diagnosis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Most patients received RASI and beta-blockers in the first months following HFrEF diagnosis. Use of ARNI, MRA and SGLT2i was limited, both in the early and later time periods. Our findings suggest that strategies to improve guideline-directed use of HFrEF therapies remain urgently needed.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"27 3\",\"pages\":\"421-431\"},\"PeriodicalIF\":16.9000,\"publicationDate\":\"2025-01-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3565\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3565\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3565","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
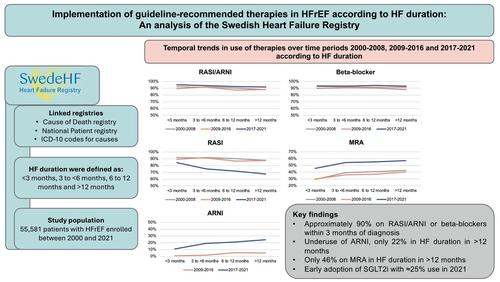
Implementation of guideline-recommended therapies in heart failure with reduced ejection fraction according to heart failure duration: An analysis of 55 581 patients from the Swedish Heart Failure (SwedeHF) Registry
Aims
Guidelines recommend immediate initiation of all four class I guideline-directed medical therapies, renin–angiotensin system inhibitors (RASI) or angiotensin receptor–neprilysin inhibitors (ARNI), beta-blockers, mineralocorticoid receptor antagonists (MRA) and sodium–glucose cotransporter 2 inhibitors (SGLT2i) following the diagnosis of heart failure (HF) with reduced ejection fraction (HFrEF). The extent to which this occurs in new-onset HFrEF is unclear. We assessed guideline-recommended therapies during the first year following a HFrEF diagnosis.
Methods and results
The Swedish HF Registry was linked to additional national registries. In patients with HFrEF (ejection fraction <40%), clinical characteristics and HF treatment from when they were available and recommended in guidelines were assessed according to time from HF diagnosis (<3, 3 to <6, 6–12 and >12 months). Of 55 581 patients with HFrEF enrolled between 2000 and 2021, 54%, 5.8%, 4.8% and 36% had an HF duration of <3, 3 to <6, 6–12 and >12 months, respectively. Patients with shorter HF duration were younger, had lower New York Heart Association class and had fewer cardiovascular comorbidities. Within 3 months, 3 to <6 months, 6–12 months and >12 months from HF diagnosis, 93%, 92%, 90% and 89% were on RASI or ARNI, 9.8%, 17%, 19% and 22% on ARNI alone, 35%, 43%, 44% and 46% on MRA, 92%, 92%, 92% and 91% on beta-blockers, and 26%, 30%, 19% and 28% on SGLT2i, respectively. Additionally, 18% received cardiac resynchronization therapy/implantable cardioverter-defibrillator >12 months after diagnosis.
Conclusions
Most patients received RASI and beta-blockers in the first months following HFrEF diagnosis. Use of ARNI, MRA and SGLT2i was limited, both in the early and later time periods. Our findings suggest that strategies to improve guideline-directed use of HFrEF therapies remain urgently needed.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


