Remy Dulery, Vincent Guiraud, Sylvain Choquet, Catherine Thieblemont, Emmanuel Bachy, Stéphane Barete, Ève Todesco, Bertrand Arnulf, Nicolas Boissel, André Baruchel, Jacques-Olivier Bay, Steven Le Gouill, Roch Houot
{"title":"CAR-T细胞治疗后的T细胞恶性肿瘤","authors":"Remy Dulery, Vincent Guiraud, Sylvain Choquet, Catherine Thieblemont, Emmanuel Bachy, Stéphane Barete, Ève Todesco, Bertrand Arnulf, Nicolas Boissel, André Baruchel, Jacques-Olivier Bay, Steven Le Gouill, Roch Houot","doi":"10.1038/s41591-024-03458-w","DOIUrl":null,"url":null,"abstract":"<p>The risk of T cell malignancies after chimeric antigen receptor (CAR) T cell therapy is a concern, although the true incidence remains unclear. Here we analyzed the DESCAR-T registry database, encompassing all pediatric and adult patients with hematologic malignancies who received CAR T cell therapy in France since 1 July 2018. Of the 3,066 patients included (2,536 B cell lymphoma, 162 B cell acute lymphoblastic leukemia (ALL) and 368 multiple myeloma), 1,680 (54.8%) received axicabtagene ciloleucel, 205 (6.7%) brexucabtagene autoleucel, 44 (1.4%) lisocabtagene maraleucel and 769 (25.1%) tisagenlecleucel. All multiple myeloma patients received idecabtagene vicleucel, with none receiving ciltacabtagene autoleucel. After a median follow-up of 12.7 months for B cell lymphoma, 17.7 months for B cell ALL and 6.3 months for multiple myeloma, only one (0.03%) patient developed a T cell malignancy after CAR T infusion. Specifically, the patient was diagnosed with a primary cutaneous CD30<sup>+</sup> T cell lymphoproliferative disorder (anaplastic lymphoma kinase-negative) 3 years after receiving tisagenlecleucel therapy for diffuse large B cell lymphoma. This was associated with the integration of a CAR clone into the tumor suppressor gene <i>PLAAT4</i> (phospholipase A and acyltransferase 4). Thus, the development of this secondary T cell malignancy might be linked to the use of CAR T cell therapy. In conclusion, our findings indicate a very low risk of T cell malignancy after CAR T cell therapy.</p>","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":"20 1","pages":""},"PeriodicalIF":58.7000,"publicationDate":"2025-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"T cell malignancies after CAR T cell therapy in the DESCAR-T registry\",\"authors\":\"Remy Dulery, Vincent Guiraud, Sylvain Choquet, Catherine Thieblemont, Emmanuel Bachy, Stéphane Barete, Ève Todesco, Bertrand Arnulf, Nicolas Boissel, André Baruchel, Jacques-Olivier Bay, Steven Le Gouill, Roch Houot\",\"doi\":\"10.1038/s41591-024-03458-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The risk of T cell malignancies after chimeric antigen receptor (CAR) T cell therapy is a concern, although the true incidence remains unclear. Here we analyzed the DESCAR-T registry database, encompassing all pediatric and adult patients with hematologic malignancies who received CAR T cell therapy in France since 1 July 2018. Of the 3,066 patients included (2,536 B cell lymphoma, 162 B cell acute lymphoblastic leukemia (ALL) and 368 multiple myeloma), 1,680 (54.8%) received axicabtagene ciloleucel, 205 (6.7%) brexucabtagene autoleucel, 44 (1.4%) lisocabtagene maraleucel and 769 (25.1%) tisagenlecleucel. All multiple myeloma patients received idecabtagene vicleucel, with none receiving ciltacabtagene autoleucel. After a median follow-up of 12.7 months for B cell lymphoma, 17.7 months for B cell ALL and 6.3 months for multiple myeloma, only one (0.03%) patient developed a T cell malignancy after CAR T infusion. Specifically, the patient was diagnosed with a primary cutaneous CD30<sup>+</sup> T cell lymphoproliferative disorder (anaplastic lymphoma kinase-negative) 3 years after receiving tisagenlecleucel therapy for diffuse large B cell lymphoma. This was associated with the integration of a CAR clone into the tumor suppressor gene <i>PLAAT4</i> (phospholipase A and acyltransferase 4). Thus, the development of this secondary T cell malignancy might be linked to the use of CAR T cell therapy. In conclusion, our findings indicate a very low risk of T cell malignancy after CAR T cell therapy.</p>\",\"PeriodicalId\":19037,\"journal\":{\"name\":\"Nature Medicine\",\"volume\":\"20 1\",\"pages\":\"\"},\"PeriodicalIF\":58.7000,\"publicationDate\":\"2025-01-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nature Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41591-024-03458-w\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"BIOCHEMISTRY & MOLECULAR BIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41591-024-03458-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
T cell malignancies after CAR T cell therapy in the DESCAR-T registry
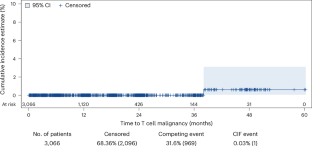
The risk of T cell malignancies after chimeric antigen receptor (CAR) T cell therapy is a concern, although the true incidence remains unclear. Here we analyzed the DESCAR-T registry database, encompassing all pediatric and adult patients with hematologic malignancies who received CAR T cell therapy in France since 1 July 2018. Of the 3,066 patients included (2,536 B cell lymphoma, 162 B cell acute lymphoblastic leukemia (ALL) and 368 multiple myeloma), 1,680 (54.8%) received axicabtagene ciloleucel, 205 (6.7%) brexucabtagene autoleucel, 44 (1.4%) lisocabtagene maraleucel and 769 (25.1%) tisagenlecleucel. All multiple myeloma patients received idecabtagene vicleucel, with none receiving ciltacabtagene autoleucel. After a median follow-up of 12.7 months for B cell lymphoma, 17.7 months for B cell ALL and 6.3 months for multiple myeloma, only one (0.03%) patient developed a T cell malignancy after CAR T infusion. Specifically, the patient was diagnosed with a primary cutaneous CD30+ T cell lymphoproliferative disorder (anaplastic lymphoma kinase-negative) 3 years after receiving tisagenlecleucel therapy for diffuse large B cell lymphoma. This was associated with the integration of a CAR clone into the tumor suppressor gene PLAAT4 (phospholipase A and acyltransferase 4). Thus, the development of this secondary T cell malignancy might be linked to the use of CAR T cell therapy. In conclusion, our findings indicate a very low risk of T cell malignancy after CAR T cell therapy.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


