{"title":"一种新的(1,3)-β- d -葡聚糖化学发光免疫分析法对侵袭性念珠菌病的评价:一项来自三级保健中心的研究","authors":"Sudesh Gourav, Gagandeep Singh, Lokesh Kashyap, Bhaskar Rana, Swet Raj, Immaculata Xess","doi":"10.22034/cmm.2024.345199.1513","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Invasive candidiasis (IC) in the hospitalized population is one of the leading causes of invasive fungal infections (IFIs). Microbiological diagnosis of IC suffers due to poor sensitivity of blood culture and relative inaccessibility to more sensitive modalities. (1, 3)-β-D-glucan (BDG) is a cell wall polysaccharide found in a range of fungi. Various commercial assays are available based on various detection techniques. This study aimed to assess the diagnostic performance of the FungiXpert® Fungus BDG Detection Kit by Genobio Pharmaceutical Co. Ltd. (Tianjin, China), based on chemiluminescent method, for diagnosis of candidemia and deep-seated candidiasis.</p><p><strong>Materials and methods: </strong>In total, 80 patients (34 males and 46 females) were included with a median age of 35 years old. In accordance with EORTC/MSGERC definitions, 39 patients had proven IC. The number of patients within the probable, possible, and no IC (taken as control) groups were 8, 4, and 29, respectively. Blood samples were collected for fungal blood culture and BDG assay.</p><p><strong>Results: </strong>After exclusion of cases with evidence of concurrent IFI other than IC, median serum BDG was 0.63 ng/ml for proven IC; while it was 0.04 ng/ml for NO IC. Sensitivity, specificity, positive, and negative predictive values were 60.52%, 81.81%, 85.18%, and 54.54%, respectively. Positive likelihood ratio was 3.32. While the assay performed best for <i>Candida tropicalis</i> with median BDG of 1.92 ng/ml and sensitivity of 92.3%, its performance was worst for <i>Candida parapsilosis</i>, with median BDG of 0.04 ng/ml and sensitivity of 44.44%. Overall mortality rate was 65.62% in the BDG positive group, which was significantly higher than that in the BDG negative group (33.33%).</p><p><strong>Conclusion: </strong>The performance of the FungiXpert® Fungus BDG Detection Kit was acceptable for invasive candidiasis in the present resource-limited setup. The major advantages of this assay were the ease of performance in a semi-automated cartridge format, relatively lower cost per test, non-reliance on glucan-free procedures or instruments and minimal hands-on procedure.</p>","PeriodicalId":10863,"journal":{"name":"Current Medical Mycology","volume":"10 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11688587/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of a newer (1, 3)-β-D-glucan chemiluminescent immunoassay for invasive candidiasis: A study from a tertiary care center.\",\"authors\":\"Sudesh Gourav, Gagandeep Singh, Lokesh Kashyap, Bhaskar Rana, Swet Raj, Immaculata Xess\",\"doi\":\"10.22034/cmm.2024.345199.1513\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>Invasive candidiasis (IC) in the hospitalized population is one of the leading causes of invasive fungal infections (IFIs). Microbiological diagnosis of IC suffers due to poor sensitivity of blood culture and relative inaccessibility to more sensitive modalities. (1, 3)-β-D-glucan (BDG) is a cell wall polysaccharide found in a range of fungi. Various commercial assays are available based on various detection techniques. This study aimed to assess the diagnostic performance of the FungiXpert® Fungus BDG Detection Kit by Genobio Pharmaceutical Co. Ltd. (Tianjin, China), based on chemiluminescent method, for diagnosis of candidemia and deep-seated candidiasis.</p><p><strong>Materials and methods: </strong>In total, 80 patients (34 males and 46 females) were included with a median age of 35 years old. In accordance with EORTC/MSGERC definitions, 39 patients had proven IC. The number of patients within the probable, possible, and no IC (taken as control) groups were 8, 4, and 29, respectively. Blood samples were collected for fungal blood culture and BDG assay.</p><p><strong>Results: </strong>After exclusion of cases with evidence of concurrent IFI other than IC, median serum BDG was 0.63 ng/ml for proven IC; while it was 0.04 ng/ml for NO IC. Sensitivity, specificity, positive, and negative predictive values were 60.52%, 81.81%, 85.18%, and 54.54%, respectively. Positive likelihood ratio was 3.32. While the assay performed best for <i>Candida tropicalis</i> with median BDG of 1.92 ng/ml and sensitivity of 92.3%, its performance was worst for <i>Candida parapsilosis</i>, with median BDG of 0.04 ng/ml and sensitivity of 44.44%. Overall mortality rate was 65.62% in the BDG positive group, which was significantly higher than that in the BDG negative group (33.33%).</p><p><strong>Conclusion: </strong>The performance of the FungiXpert® Fungus BDG Detection Kit was acceptable for invasive candidiasis in the present resource-limited setup. The major advantages of this assay were the ease of performance in a semi-automated cartridge format, relatively lower cost per test, non-reliance on glucan-free procedures or instruments and minimal hands-on procedure.</p>\",\"PeriodicalId\":10863,\"journal\":{\"name\":\"Current Medical Mycology\",\"volume\":\"10 \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-05-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11688587/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Medical Mycology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22034/cmm.2024.345199.1513\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Medical Mycology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22034/cmm.2024.345199.1513","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景与目的:侵袭性念珠菌病(IC)在住院人群中是侵袭性真菌感染(IFIs)的主要原因之一。由于血液培养的敏感性较差和相对难以获得更敏感的模式,IC的微生物诊断受到影响。(1,3)-β- d -葡聚糖(BDG)是一种存在于多种真菌中的细胞壁多糖。基于各种检测技术的各种商业分析是可用的。本研究旨在评价天津Genobio制药有限公司基于化学发光法的FungiXpert®真菌BDG检测试剂盒对念珠菌病和深部念珠菌病的诊断效果。材料与方法:共纳入80例患者,其中男34例,女46例,中位年龄35岁。根据EORTC/MSGERC的定义,39例患者被证实为IC。可能组、可能组和非IC组(作为对照)的患者分别为8例、4例和29例。采集血样进行真菌血培养和BDG检测。结果:在排除除IC外有其他IFI证据的病例后,证实IC的中位血清BDG为0.63 ng/ml;NO IC为0.04 ng/ml,敏感性为60.52%,特异性为81.81%,阳性预测值为85.18%,阴性预测值为54.54%。正似然比为3.32。该方法对热带假丝酵母检测效果最好,BDG中位数为1.92 ng/ml,灵敏度为92.3%;对假丝酵母检测效果最差,BDG中位数为0.04 ng/ml,灵敏度为44.44%。BDG阳性组总死亡率为65.62%,显著高于BDG阴性组(33.33%)。结论:在目前资源有限的条件下,FungiXpert®真菌BDG检测试剂盒对侵袭性念珠菌病的检测性能是可以接受的。该分析的主要优点是易于在半自动化盒格式中进行,每次测试的成本相对较低,不依赖于无葡聚糖程序或仪器,并且最少的动手程序。
Evaluation of a newer (1, 3)-β-D-glucan chemiluminescent immunoassay for invasive candidiasis: A study from a tertiary care center.
Background and purpose: Invasive candidiasis (IC) in the hospitalized population is one of the leading causes of invasive fungal infections (IFIs). Microbiological diagnosis of IC suffers due to poor sensitivity of blood culture and relative inaccessibility to more sensitive modalities. (1, 3)-β-D-glucan (BDG) is a cell wall polysaccharide found in a range of fungi. Various commercial assays are available based on various detection techniques. This study aimed to assess the diagnostic performance of the FungiXpert® Fungus BDG Detection Kit by Genobio Pharmaceutical Co. Ltd. (Tianjin, China), based on chemiluminescent method, for diagnosis of candidemia and deep-seated candidiasis.
Materials and methods: In total, 80 patients (34 males and 46 females) were included with a median age of 35 years old. In accordance with EORTC/MSGERC definitions, 39 patients had proven IC. The number of patients within the probable, possible, and no IC (taken as control) groups were 8, 4, and 29, respectively. Blood samples were collected for fungal blood culture and BDG assay.
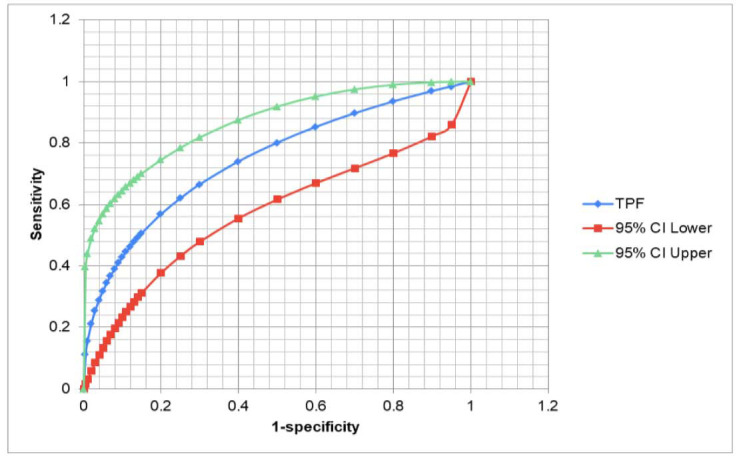
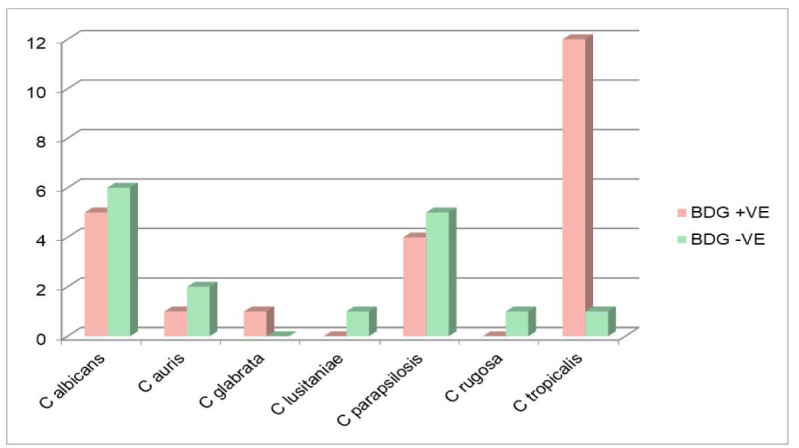
Results: After exclusion of cases with evidence of concurrent IFI other than IC, median serum BDG was 0.63 ng/ml for proven IC; while it was 0.04 ng/ml for NO IC. Sensitivity, specificity, positive, and negative predictive values were 60.52%, 81.81%, 85.18%, and 54.54%, respectively. Positive likelihood ratio was 3.32. While the assay performed best for Candida tropicalis with median BDG of 1.92 ng/ml and sensitivity of 92.3%, its performance was worst for Candida parapsilosis, with median BDG of 0.04 ng/ml and sensitivity of 44.44%. Overall mortality rate was 65.62% in the BDG positive group, which was significantly higher than that in the BDG negative group (33.33%).
Conclusion: The performance of the FungiXpert® Fungus BDG Detection Kit was acceptable for invasive candidiasis in the present resource-limited setup. The major advantages of this assay were the ease of performance in a semi-automated cartridge format, relatively lower cost per test, non-reliance on glucan-free procedures or instruments and minimal hands-on procedure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


