Gian Jacobs, Kate Emblin, Umesh Kadam, Rob Daniels, Mohammad Alallan, Kinan Mokbel
{"title":"非依从性房颤患者肺栓塞掩盖心力衰竭:病例报告和文献分析综述。","authors":"Gian Jacobs, Kate Emblin, Umesh Kadam, Rob Daniels, Mohammad Alallan, Kinan Mokbel","doi":"10.21873/invivo.13859","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Atrial fibrillation (AF) and heart failure (HF) commonly co-occur, significantly increasing morbidity and mortality. Poorly controlled AF can contribute to complications like HF and is associated with conditions, such as stroke and pulmonary embolism (PE). This report involves a man with AF who had persistent respiratory symptoms and left-sided chest pain, initially suspected to be PE, but eventually diagnosed as HF.</p><p><strong>Case report: </strong>A 43-year-old male experienced increasing breathlessness, cough, and fatigue. Initially suspected to have a respiratory infection, his persistent symptoms raised concern for PE. The patient had a history of AF, unsuccessful cardioversion, and long-term non-adherence to beta blockers. Initial assessment revealed persistent respiratory symptoms and elevated levels of C-reactive protein, D-dimer, N-terminal pro-B-type natriuretic peptide, and Troponin T. Chest X-ray showed pulmonary congestion, and echocardiogram confirmed a severely impaired ejection fraction (EF <20%). While the differential diagnosis included community-acquired pneumonia, PE, and HF, the final diagnosis was worsening AF and HF with reduced EF, not PE.</p><p><strong>Conclusion: </strong>PE symptoms can overlap with HF, making careful differential diagnosis essential, particularly in AF patients with elevated D-dimer levels, where false positives necessitate caution. This case underscores the importance of thorough differential diagnosis and clinical judgment before ordering tests to avoid misdiagnosis. Long-term non-adherence to beta blockers exacerbated the patient's symptoms, emphasising the critical role of consistent medication use in managing AF and preventing complications like HF. This case report also highlights the importance of thorough investigations, guideline-based treatments and multidisciplinary care in complex AF-HF cases.</p>","PeriodicalId":13364,"journal":{"name":"In vivo","volume":"39 1","pages":"548-558"},"PeriodicalIF":1.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11705105/pdf/","citationCount":"0","resultStr":"{\"title\":\"Heart Failure Masked as Pulmonary Embolism in Non-adherent Patient With Atrial Fibrillation: Case Report and Analytical Review of the Literature.\",\"authors\":\"Gian Jacobs, Kate Emblin, Umesh Kadam, Rob Daniels, Mohammad Alallan, Kinan Mokbel\",\"doi\":\"10.21873/invivo.13859\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/aim: </strong>Atrial fibrillation (AF) and heart failure (HF) commonly co-occur, significantly increasing morbidity and mortality. Poorly controlled AF can contribute to complications like HF and is associated with conditions, such as stroke and pulmonary embolism (PE). This report involves a man with AF who had persistent respiratory symptoms and left-sided chest pain, initially suspected to be PE, but eventually diagnosed as HF.</p><p><strong>Case report: </strong>A 43-year-old male experienced increasing breathlessness, cough, and fatigue. Initially suspected to have a respiratory infection, his persistent symptoms raised concern for PE. The patient had a history of AF, unsuccessful cardioversion, and long-term non-adherence to beta blockers. Initial assessment revealed persistent respiratory symptoms and elevated levels of C-reactive protein, D-dimer, N-terminal pro-B-type natriuretic peptide, and Troponin T. Chest X-ray showed pulmonary congestion, and echocardiogram confirmed a severely impaired ejection fraction (EF <20%). While the differential diagnosis included community-acquired pneumonia, PE, and HF, the final diagnosis was worsening AF and HF with reduced EF, not PE.</p><p><strong>Conclusion: </strong>PE symptoms can overlap with HF, making careful differential diagnosis essential, particularly in AF patients with elevated D-dimer levels, where false positives necessitate caution. This case underscores the importance of thorough differential diagnosis and clinical judgment before ordering tests to avoid misdiagnosis. Long-term non-adherence to beta blockers exacerbated the patient's symptoms, emphasising the critical role of consistent medication use in managing AF and preventing complications like HF. This case report also highlights the importance of thorough investigations, guideline-based treatments and multidisciplinary care in complex AF-HF cases.</p>\",\"PeriodicalId\":13364,\"journal\":{\"name\":\"In vivo\",\"volume\":\"39 1\",\"pages\":\"548-558\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11705105/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"In vivo\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21873/invivo.13859\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"In vivo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21873/invivo.13859","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Heart Failure Masked as Pulmonary Embolism in Non-adherent Patient With Atrial Fibrillation: Case Report and Analytical Review of the Literature.
Background/aim: Atrial fibrillation (AF) and heart failure (HF) commonly co-occur, significantly increasing morbidity and mortality. Poorly controlled AF can contribute to complications like HF and is associated with conditions, such as stroke and pulmonary embolism (PE). This report involves a man with AF who had persistent respiratory symptoms and left-sided chest pain, initially suspected to be PE, but eventually diagnosed as HF.
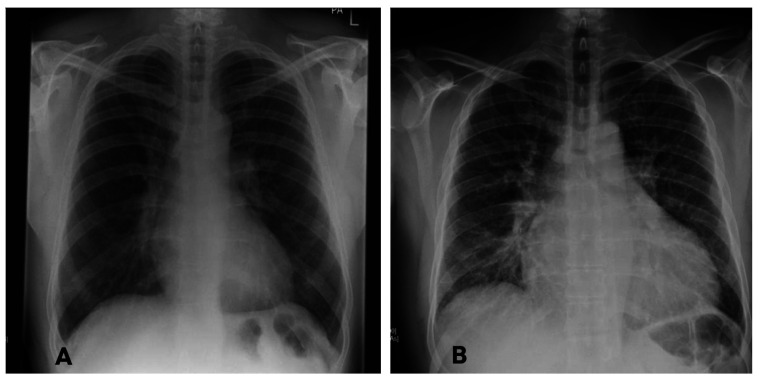
Case report: A 43-year-old male experienced increasing breathlessness, cough, and fatigue. Initially suspected to have a respiratory infection, his persistent symptoms raised concern for PE. The patient had a history of AF, unsuccessful cardioversion, and long-term non-adherence to beta blockers. Initial assessment revealed persistent respiratory symptoms and elevated levels of C-reactive protein, D-dimer, N-terminal pro-B-type natriuretic peptide, and Troponin T. Chest X-ray showed pulmonary congestion, and echocardiogram confirmed a severely impaired ejection fraction (EF <20%). While the differential diagnosis included community-acquired pneumonia, PE, and HF, the final diagnosis was worsening AF and HF with reduced EF, not PE.
Conclusion: PE symptoms can overlap with HF, making careful differential diagnosis essential, particularly in AF patients with elevated D-dimer levels, where false positives necessitate caution. This case underscores the importance of thorough differential diagnosis and clinical judgment before ordering tests to avoid misdiagnosis. Long-term non-adherence to beta blockers exacerbated the patient's symptoms, emphasising the critical role of consistent medication use in managing AF and preventing complications like HF. This case report also highlights the importance of thorough investigations, guideline-based treatments and multidisciplinary care in complex AF-HF cases.
期刊介绍:
IN VIVO is an international peer-reviewed journal designed to bring together original high quality works and reviews on experimental and clinical biomedical research within the frames of physiology, pathology and disease management.
The topics of IN VIVO include: 1. Experimental development and application of new diagnostic and therapeutic procedures; 2. Pharmacological and toxicological evaluation of new drugs, drug combinations and drug delivery systems; 3. Clinical trials; 4. Development and characterization of models of biomedical research; 5. Cancer diagnosis and treatment; 6. Immunotherapy and vaccines; 7. Radiotherapy, Imaging; 8. Tissue engineering, Regenerative medicine; 9. Carcinogenesis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



