长期转移性甲状腺髓样癌引起全身降钙素淀粉样变的并发症:肾病综合征。
IF 1.2
Q3 Medicine
引用次数: 0
摘要
背景/目的:甲状腺髓样癌常导致降钙素水平升高,可引起局部降钙素淀粉样蛋白的形成,但很少有系统性降钙素淀粉样变的并发症报道。本报告的目的是鼓励认识降钙素淀粉样蛋白引起肾病综合征的转移性甲状腺髓样癌患者。病例报告:65岁女性,虚弱,乏力,贫血,血小板减少,静脉和动脉血栓,右肺空洞性病变转院治疗。她有14年的转移性甲状腺髓样癌病史,甲状腺切除术和酪氨酸激酶抑制剂治疗后的状态,促肾上腺皮质激素依赖性库欣综合征缓解,最近诊断为肾病综合征。入院时,患者有下肢水肿和散在性瘀斑。实验结果:肌酐0.62 mg/dL (0.7 ~ 1.3 mg/dL),晨间皮质醇>119.6 ug/dL (4 ~ 23 ug/dL),促肾上腺皮质激素426 pg/mL (6 ~ 50 pg/mL), 24小时尿皮质醇6115.2 mcg/24 h (4 ~ 50 mcg/24 h),降钙素39 373 pg/mL(≤5 pg/mL),癌胚抗原484.8 ng/mL (0 ~ 4.9 ng/mL)。肾活检显示淀粉样变,降钙素染色阳性。讨论:全身性降钙素淀粉样变在甲状腺髓样癌中没有充分的证据。据我们所知,先前有2例病例报告描述了甲状腺髓样癌中继发于降钙素淀粉样蛋白的肾病综合征。结论:本病例支持少量证据表明转移性甲状腺髓样癌可导致全身降钙素淀粉样变及其并发症,包括肾病综合征。临床医生应考虑肾病综合征作为转移性甲状腺髓样癌患者的潜在并发症,特别是那些长期降钙素升高和特征性症状的患者。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Nephrotic Syndrome as a Complication of Systemic Calcitonin Amyloidosis From Long-Standing Metastatic Medullary Thyroid Cancer
Background/Objective
Medullary thyroid cancer often results in elevated calcitonin levels, which can cause localized formation of calcitonin amyloid, though rarely complications of systemic calcitonin amyloidosis have been reported. The objective of this report is to encourage awareness of calcitonin amyloid causing nephrotic syndrome in patients with metastatic medullary thyroid cancer.
Case Report
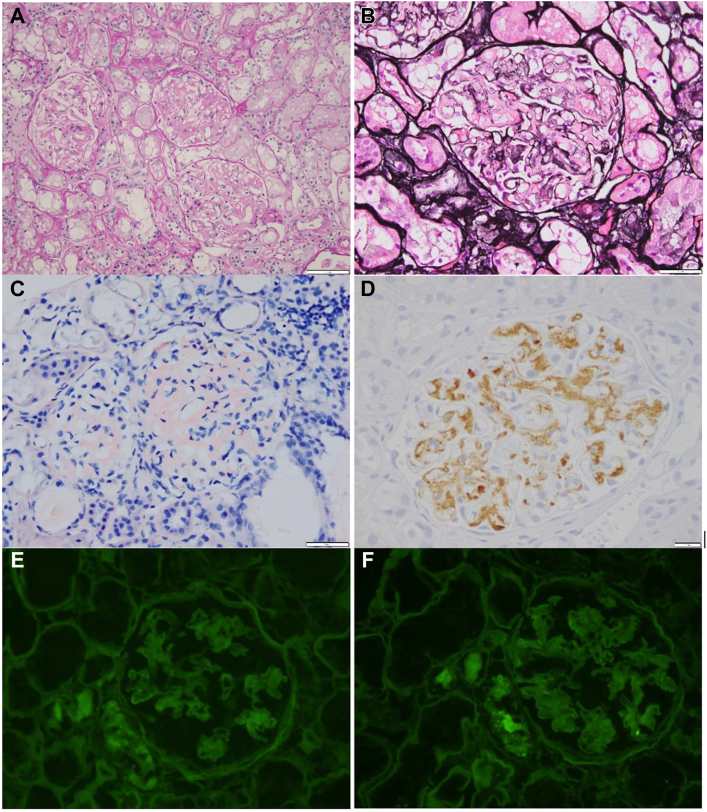
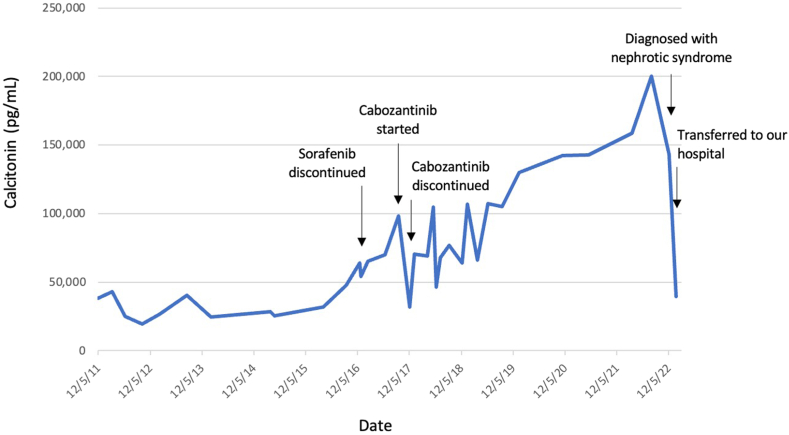
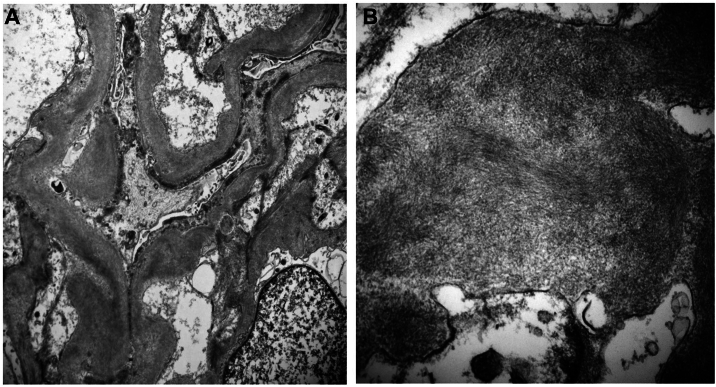
A 65-year-old woman with weakness, fatigue, anasarca, anemia, thrombocytopenia, venous and arterial thrombi, and a cavitary right lung lesion was transferred for care. She had a 14-year history of metastatic medullary thyroid cancer, status post-thyroidectomy and tyrosine kinase inhibitor therapy, adrenocorticotropic hormone-dependent Cushing syndrome in remission, and recently diagnosed nephrotic syndrome. On admission, she had lower extremity edema and scattered ecchymoses. Labs showed creatinine 0.62 mg/dL (0.7-1.3 mg/dL), morning cortisol >119.6 ug/dL (4-23 ug/dL), adrenocorticotropic hormone 426 pg/mL (6-50 pg/mL), 24-hour urine cortisol 6115.2 mcg/24 h (4-50 mcg/24 h), calcitonin 39 373 pg/mL (≤5 pg/mL), and carcinoembryonic antigen level 484.8 ng/mL (0-4.9 ng/mL). Kidney biopsy showed amyloidosis, which stained positive for calcitonin.
Discussion
Systemic calcitonin amyloidosis is not well-documented in medullary thyroid cancer. To our knowledge, there are 2 previous case reports describing nephrotic syndrome secondary to calcitonin amyloid in the setting of medullary thyroid cancer.
Conclusion
This case supports a small body of evidence that metastatic medullary thyroid cancer can result in systemic calcitonin amyloidosis and its complications, including nephrotic syndrome. Clinicians should consider nephrotic syndrome as a potential complication in patients with metastatic medullary thyroid cancer, particularly in those with long-standing calcitonin elevation and characteristic symptoms.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

AACE Clinical Case Reports
Medicine-Endocrinology, Diabetes and Metabolism
CiteScore
2.30
自引率
0.00%
发文量
61
审稿时长
55 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


