Alba Gabaldon-Albero, Carla Martin-Grau, Miguel Marti-Masanet, Alejandro Lopez-Jimenez, Roberto Llorens, Beatriz Beseler-Soto, Sergio Martin-Zamora, Berta Lopez, Inmaculada Calvo, Sara Hernandez-Muela, Monica Rosello, Carmen Orellana, Francisco Martinez
{"title":"6型aicardii - gouti<e:1>综合征:新生儿期ruxolitinib治疗后ADAR变异及临床结果报告","authors":"Alba Gabaldon-Albero, Carla Martin-Grau, Miguel Marti-Masanet, Alejandro Lopez-Jimenez, Roberto Llorens, Beatriz Beseler-Soto, Sergio Martin-Zamora, Berta Lopez, Inmaculada Calvo, Sara Hernandez-Muela, Monica Rosello, Carmen Orellana, Francisco Martinez","doi":"10.1186/s12969-024-01036-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Aicardi-Goutières Syndrome is a monogenic type 1 interferonopathy with infantile onset, characterized by a variable degree of neurological damage. Approximately 7% of Aicardi-Goutières Syndrome cases are caused by pathogenic variants in the ADAR gene and are classified as Aicardi-Goutières Syndrome type 6. Here, we present a new homozygous pathogenic variant in the ADAR gene. Currently, Janus Kinase inhibitors have been proposed to treat selected interferonopathies such as Aicardi-Goutières Syndrome, although limited information is available on its use and results in the neonatal presentation of this disease.</p><p><strong>Case presentation: </strong>We present two siblings, a male neonate with congenital petechial rash, severe thrombopenia and generalized hypotonia and his deceased sister who had normal development until 5 months of age, when she suffered acute encephalopathy. We describe the clinical course, complementary examinations and follow-up with early treatment of the newborn with ruxolitinib. The homozygous variant c.2908G > A (p.Ala970Thr) in the ADAR gene was found in both siblings, parents were heterozygous carriers.</p><p><strong>Conclusions: </strong>The homozygous variant c.2908G > A (p.Ala970Thr) in the ADAR gene causes Aicardi-Goutières Syndrome type 6. Intrafamilial phenotypic spectrum of the disease varies among individuals with the same pathogenic variant. Early initiation of ruxolitinib improved systemic signs but did not prevent the progression of neurological disease.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"22 1","pages":"110"},"PeriodicalIF":2.3000,"publicationDate":"2024-12-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11682636/pdf/","citationCount":"0","resultStr":"{\"title\":\"Aicardi-Goutières syndrome type 6: report of ADAR variant and clinical outcome after ruxolitinib treatment in the neonatal period.\",\"authors\":\"Alba Gabaldon-Albero, Carla Martin-Grau, Miguel Marti-Masanet, Alejandro Lopez-Jimenez, Roberto Llorens, Beatriz Beseler-Soto, Sergio Martin-Zamora, Berta Lopez, Inmaculada Calvo, Sara Hernandez-Muela, Monica Rosello, Carmen Orellana, Francisco Martinez\",\"doi\":\"10.1186/s12969-024-01036-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Aicardi-Goutières Syndrome is a monogenic type 1 interferonopathy with infantile onset, characterized by a variable degree of neurological damage. Approximately 7% of Aicardi-Goutières Syndrome cases are caused by pathogenic variants in the ADAR gene and are classified as Aicardi-Goutières Syndrome type 6. Here, we present a new homozygous pathogenic variant in the ADAR gene. Currently, Janus Kinase inhibitors have been proposed to treat selected interferonopathies such as Aicardi-Goutières Syndrome, although limited information is available on its use and results in the neonatal presentation of this disease.</p><p><strong>Case presentation: </strong>We present two siblings, a male neonate with congenital petechial rash, severe thrombopenia and generalized hypotonia and his deceased sister who had normal development until 5 months of age, when she suffered acute encephalopathy. We describe the clinical course, complementary examinations and follow-up with early treatment of the newborn with ruxolitinib. The homozygous variant c.2908G > A (p.Ala970Thr) in the ADAR gene was found in both siblings, parents were heterozygous carriers.</p><p><strong>Conclusions: </strong>The homozygous variant c.2908G > A (p.Ala970Thr) in the ADAR gene causes Aicardi-Goutières Syndrome type 6. Intrafamilial phenotypic spectrum of the disease varies among individuals with the same pathogenic variant. Early initiation of ruxolitinib improved systemic signs but did not prevent the progression of neurological disease.</p>\",\"PeriodicalId\":54630,\"journal\":{\"name\":\"Pediatric Rheumatology\",\"volume\":\"22 1\",\"pages\":\"110\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-12-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11682636/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Rheumatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12969-024-01036-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-024-01036-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
Aicardi-Goutières syndrome type 6: report of ADAR variant and clinical outcome after ruxolitinib treatment in the neonatal period.
Background: Aicardi-Goutières Syndrome is a monogenic type 1 interferonopathy with infantile onset, characterized by a variable degree of neurological damage. Approximately 7% of Aicardi-Goutières Syndrome cases are caused by pathogenic variants in the ADAR gene and are classified as Aicardi-Goutières Syndrome type 6. Here, we present a new homozygous pathogenic variant in the ADAR gene. Currently, Janus Kinase inhibitors have been proposed to treat selected interferonopathies such as Aicardi-Goutières Syndrome, although limited information is available on its use and results in the neonatal presentation of this disease.
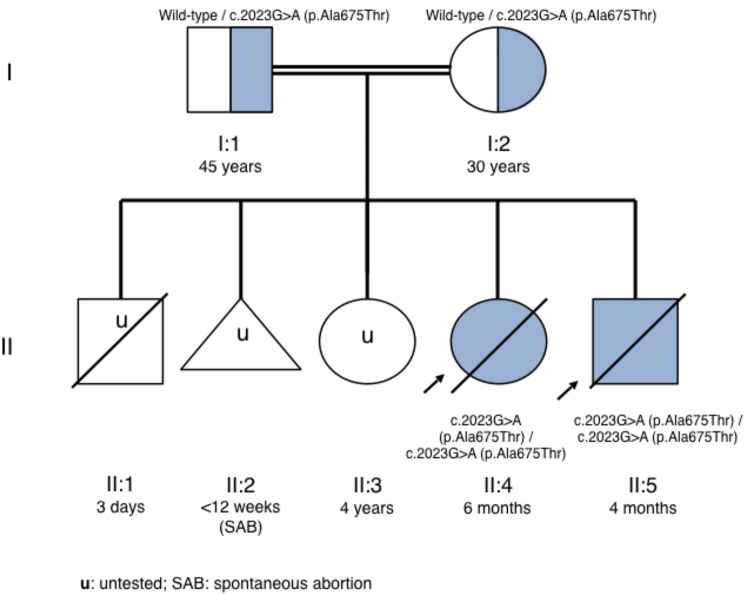
Case presentation: We present two siblings, a male neonate with congenital petechial rash, severe thrombopenia and generalized hypotonia and his deceased sister who had normal development until 5 months of age, when she suffered acute encephalopathy. We describe the clinical course, complementary examinations and follow-up with early treatment of the newborn with ruxolitinib. The homozygous variant c.2908G > A (p.Ala970Thr) in the ADAR gene was found in both siblings, parents were heterozygous carriers.
Conclusions: The homozygous variant c.2908G > A (p.Ala970Thr) in the ADAR gene causes Aicardi-Goutières Syndrome type 6. Intrafamilial phenotypic spectrum of the disease varies among individuals with the same pathogenic variant. Early initiation of ruxolitinib improved systemic signs but did not prevent the progression of neurological disease.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


