米索前列醇诱导子宫破裂治疗妊娠中期宫内死胎1例。
IF 0.6
Q4 OBSTETRICS & GYNECOLOGY
引用次数: 0
摘要
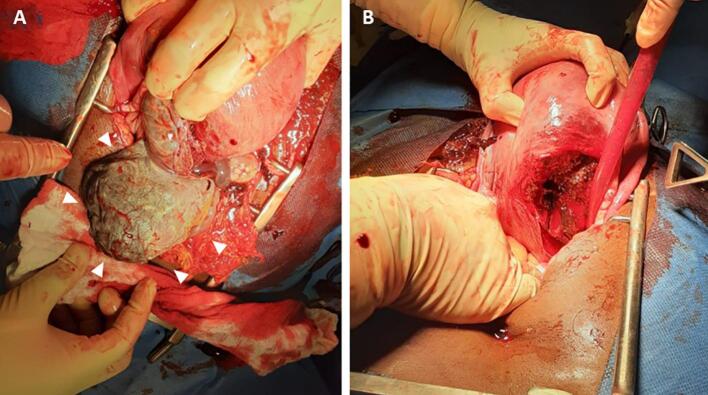
子宫破裂是使用米索前列醇的一个众所周知的危及生命的并发症;发病率非常低。在这里,我们报告什么似乎是第一个记录的情况下,引产后宫内胎儿死亡宫内妊娠中期子宫破裂无子宫疤痕。女性,40岁,无剖宫产史,无子宫手术史。经腹超声检查显示胎儿宫内死亡,推测胎龄为20周。米索前列醇给药3次,每小时400 μg,服药2小时,患者主诉腹痛;然而,胎儿并没有被排出体外。重复超声显示胎儿在腹腔和骨盆积液。基于可能的诊断子宫破裂,进行剖腹手术。腹内出血量约250-300毫升。子宫后壁有一个约10厘米长的线状破裂,结果在腹腔内发现浸渍和腐臭的胎儿和部分胎盘。患者行全子宫切除术,干预3天后出院,无术后并发症。总之,虽然米索前列醇用于中期妊娠终止通常是安全的,但在子宫炎症的情况下应谨慎使用并密切监测。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Uterine rupture with induction using misoprostol for intrauterine foetal death in the second trimester: A case report
Uterine rupture is a well-known, life-threatening complication of misoprostol use; the incidence is remarkably low. Herein, we report what seems to be the first documented case of uterine rupture following induction of labour for intrauterine foetal death in the second trimester without a uterine scar. A 40-year-old woman with no history of caesarean section or uterine surgery presented with mild lower abdominal pain and mild genital bleeding. Transabdominal ultrasonography revealed intrauterine foetal death, at presumed gestational age of 20 weeks. Two hours after three doses of 400 μg 3-hourly of misoprostol, the patient complained of abdominal pain; however, the foetus was not expelled. Repeat sonography revealed the foetus in the abdominal cavity and fluid collection in the pelvis. Based on the probable diagnosis of uterine rupture, a laparotomy was performed. The intra-abdominal haemorrhage volume was approximately 250–300 ml. There was a linear rupture approximately 10 cm long on the posterior wall of the uterus, and as a consequence, a macerated and foetid foetus and part of the placenta were found in the abdominal cavity. A total hysterectomy was performed, and the patient was discharged three days after the intervention without any postoperative complications. In conclusion, while misoprostol is generally safe for second-trimester pregnancy termination, its use should be approached with caution and close monitoring in cases of uterine inflammation.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Case Reports in Women's Health
Medicine-Obstetrics and Gynecology
CiteScore
2.10
自引率
0.00%
发文量
89
审稿时长
7 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


