Alberto Nordmann-Gomes, Gabriel Cojuc-Konigsberg, Adriana Hernández-Andrade, Valeria Navarro-Sánchez, Juan Carlos Ramírez-Sandoval, Brad Rovin, Juan M Mejia-Vilet
{"title":"狼疮肾炎随机对照试验:证据差距和代表性不足的群体。","authors":"Alberto Nordmann-Gomes, Gabriel Cojuc-Konigsberg, Adriana Hernández-Andrade, Valeria Navarro-Sánchez, Juan Carlos Ramírez-Sandoval, Brad Rovin, Juan M Mejia-Vilet","doi":"10.1136/lupus-2024-001331","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We performed a scoping review of randomised clinical trials (RCTs) assessing pharmacological therapies for the initial management of lupus nephritis (LN), focusing on study design, included populations and outcome definitions, to assess the generalisability of their results and identify gaps in the evidence.</p><p><strong>Methods: </strong>RCTs evaluating pharmacological interventions for the initial therapy of LN published between 2000 and 2024 were evaluated. Extracted variables included study design, selection criteria, outcome definitions, populations recruited and clinical characteristics of participants. Each study arm was included as intervention and segregated into guideline-recommended regimens (cyclophosphamide (CYC), mycophenolic acid analogues (MPAAs), calcineurin inhibitors and belimumab) or other regimens. Data were analysed by descriptive statistics, and Fragility Index (FI) was estimated to assess robustness of studies.</p><p><strong>Results: </strong>We included 124 intervention arms within 61 RCT, involving 7058 participants. Seventy-nine arms (63.7%) corresponded to guideline-recommended therapies: 33 (26.6%) MPAA, 28 (22.6%) NIH-CYC and 7 (5.6%) triple-drug therapies. While 100% of triple-drug therapies RCT were multinational, only 7.1% of NIH-CYC and 0% of tacrolimus RCTs were conducted in more than one country. Only 9 (14.8%) had follow-up ≥24 months. Ten (16.4%) RCTs exclusively included participants with severe or refractory LN. Only 29 (47.5%) reported serious adverse events, and few described patient-reported outcomes. Black and other race participants were under-represented, as well as participants from Middle East, North Africa, and the sub-Saharan African region. Response was variably defined and assessed at different intervals. Robustness of RCTs evaluating double-drug guideline-recommended therapies were mostly low, with FI ranging from 1 to 3.</p><p><strong>Conclusions: </strong>Considering new recommendations for the management of LN, we call for broader inclusion of under-represented populations and homogenisation of study design. This study provides the rationale for evaluating unexplored treatment comparisons and conducting research on newer interventions in clinical settings where evidence is currently lacking.</p>","PeriodicalId":18126,"journal":{"name":"Lupus Science & Medicine","volume":"11 2","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11664369/pdf/","citationCount":"0","resultStr":"{\"title\":\"Lupus nephritis randomised controlled trials: evidence gaps and under-represented groups.\",\"authors\":\"Alberto Nordmann-Gomes, Gabriel Cojuc-Konigsberg, Adriana Hernández-Andrade, Valeria Navarro-Sánchez, Juan Carlos Ramírez-Sandoval, Brad Rovin, Juan M Mejia-Vilet\",\"doi\":\"10.1136/lupus-2024-001331\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>We performed a scoping review of randomised clinical trials (RCTs) assessing pharmacological therapies for the initial management of lupus nephritis (LN), focusing on study design, included populations and outcome definitions, to assess the generalisability of their results and identify gaps in the evidence.</p><p><strong>Methods: </strong>RCTs evaluating pharmacological interventions for the initial therapy of LN published between 2000 and 2024 were evaluated. Extracted variables included study design, selection criteria, outcome definitions, populations recruited and clinical characteristics of participants. Each study arm was included as intervention and segregated into guideline-recommended regimens (cyclophosphamide (CYC), mycophenolic acid analogues (MPAAs), calcineurin inhibitors and belimumab) or other regimens. Data were analysed by descriptive statistics, and Fragility Index (FI) was estimated to assess robustness of studies.</p><p><strong>Results: </strong>We included 124 intervention arms within 61 RCT, involving 7058 participants. Seventy-nine arms (63.7%) corresponded to guideline-recommended therapies: 33 (26.6%) MPAA, 28 (22.6%) NIH-CYC and 7 (5.6%) triple-drug therapies. While 100% of triple-drug therapies RCT were multinational, only 7.1% of NIH-CYC and 0% of tacrolimus RCTs were conducted in more than one country. Only 9 (14.8%) had follow-up ≥24 months. Ten (16.4%) RCTs exclusively included participants with severe or refractory LN. Only 29 (47.5%) reported serious adverse events, and few described patient-reported outcomes. Black and other race participants were under-represented, as well as participants from Middle East, North Africa, and the sub-Saharan African region. Response was variably defined and assessed at different intervals. Robustness of RCTs evaluating double-drug guideline-recommended therapies were mostly low, with FI ranging from 1 to 3.</p><p><strong>Conclusions: </strong>Considering new recommendations for the management of LN, we call for broader inclusion of under-represented populations and homogenisation of study design. This study provides the rationale for evaluating unexplored treatment comparisons and conducting research on newer interventions in clinical settings where evidence is currently lacking.</p>\",\"PeriodicalId\":18126,\"journal\":{\"name\":\"Lupus Science & Medicine\",\"volume\":\"11 2\",\"pages\":\"\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-12-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11664369/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Lupus Science & Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/lupus-2024-001331\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lupus Science & Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/lupus-2024-001331","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Lupus nephritis randomised controlled trials: evidence gaps and under-represented groups.
Objective: We performed a scoping review of randomised clinical trials (RCTs) assessing pharmacological therapies for the initial management of lupus nephritis (LN), focusing on study design, included populations and outcome definitions, to assess the generalisability of their results and identify gaps in the evidence.
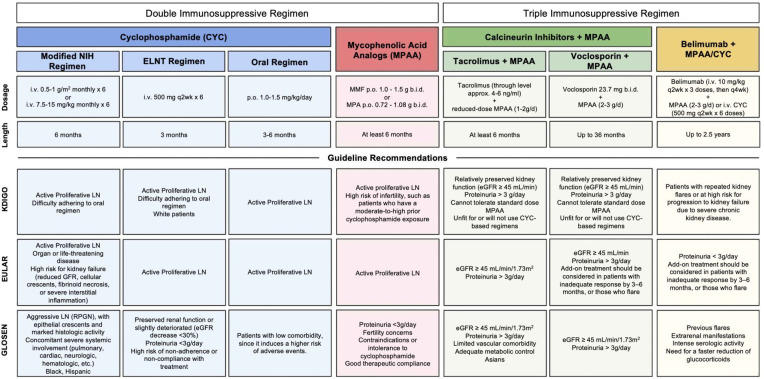
Methods: RCTs evaluating pharmacological interventions for the initial therapy of LN published between 2000 and 2024 were evaluated. Extracted variables included study design, selection criteria, outcome definitions, populations recruited and clinical characteristics of participants. Each study arm was included as intervention and segregated into guideline-recommended regimens (cyclophosphamide (CYC), mycophenolic acid analogues (MPAAs), calcineurin inhibitors and belimumab) or other regimens. Data were analysed by descriptive statistics, and Fragility Index (FI) was estimated to assess robustness of studies.
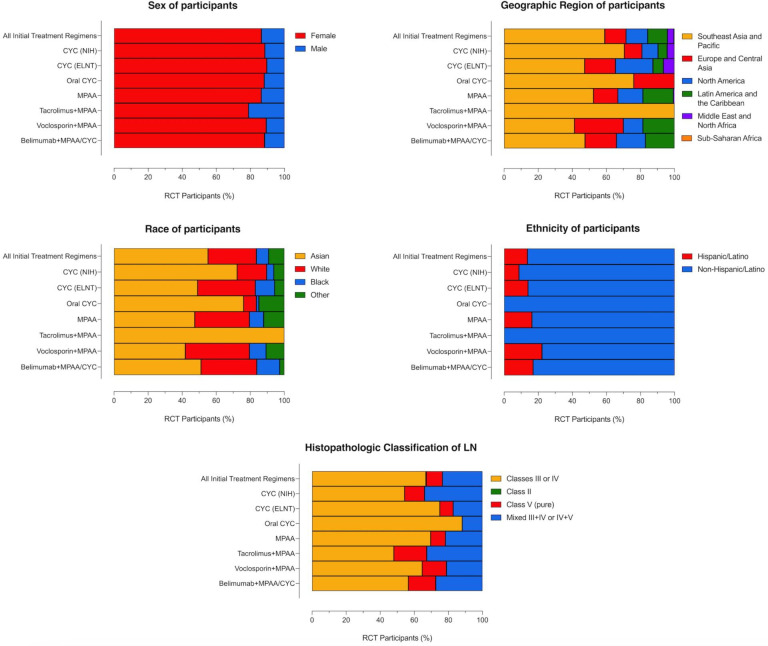
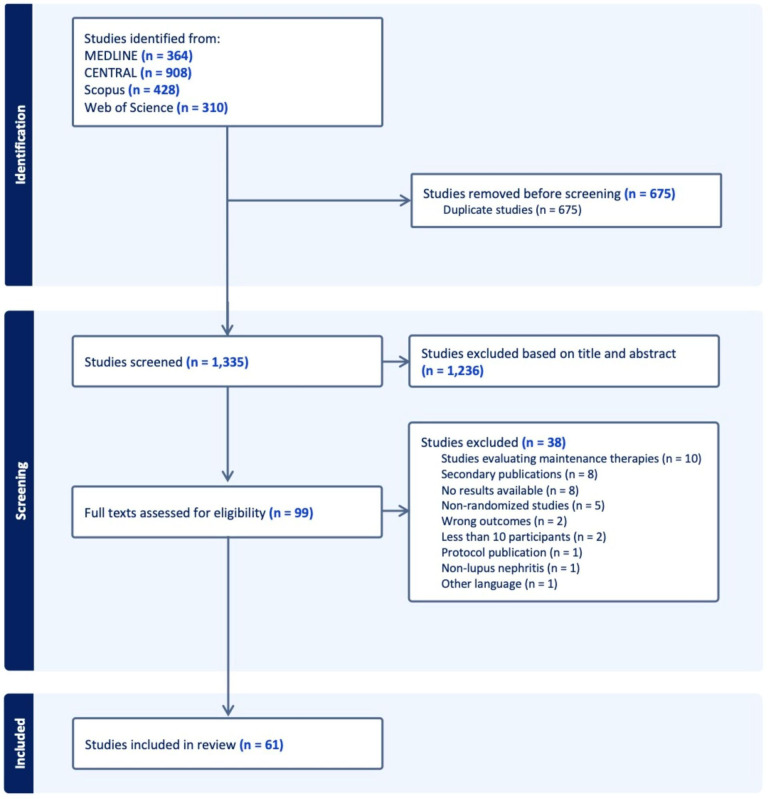
Results: We included 124 intervention arms within 61 RCT, involving 7058 participants. Seventy-nine arms (63.7%) corresponded to guideline-recommended therapies: 33 (26.6%) MPAA, 28 (22.6%) NIH-CYC and 7 (5.6%) triple-drug therapies. While 100% of triple-drug therapies RCT were multinational, only 7.1% of NIH-CYC and 0% of tacrolimus RCTs were conducted in more than one country. Only 9 (14.8%) had follow-up ≥24 months. Ten (16.4%) RCTs exclusively included participants with severe or refractory LN. Only 29 (47.5%) reported serious adverse events, and few described patient-reported outcomes. Black and other race participants were under-represented, as well as participants from Middle East, North Africa, and the sub-Saharan African region. Response was variably defined and assessed at different intervals. Robustness of RCTs evaluating double-drug guideline-recommended therapies were mostly low, with FI ranging from 1 to 3.
Conclusions: Considering new recommendations for the management of LN, we call for broader inclusion of under-represented populations and homogenisation of study design. This study provides the rationale for evaluating unexplored treatment comparisons and conducting research on newer interventions in clinical settings where evidence is currently lacking.
期刊介绍:
Lupus Science & Medicine is a global, peer reviewed, open access online journal that provides a central point for publication of basic, clinical, translational, and epidemiological studies of all aspects of lupus and related diseases. It is the first lupus-specific open access journal in the world and was developed in response to the need for a barrier-free forum for publication of groundbreaking studies in lupus. The journal publishes research on lupus from fields including, but not limited to: rheumatology, dermatology, nephrology, immunology, pediatrics, cardiology, hepatology, pulmonology, obstetrics and gynecology, and psychiatry.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


