Andres E Daryanani, Muhannad A Abbasi, Maria F Gomez Ardila, Eduardo Tellez-Garcia, Juan M Garzon-Dangond, Yi Lin, Jonas Paludo, Joerg Herrmann, Stephen M Ansell, Allison C Rosenthal, Hector R Villarraga
{"title":"基线超声心动图变量作为血液动力学显著细胞因子释放综合征的预测因子在成人接受CD19 CAR - t细胞治疗的血液恶性肿瘤。","authors":"Andres E Daryanani, Muhannad A Abbasi, Maria F Gomez Ardila, Eduardo Tellez-Garcia, Juan M Garzon-Dangond, Yi Lin, Jonas Paludo, Joerg Herrmann, Stephen M Ansell, Allison C Rosenthal, Hector R Villarraga","doi":"10.1186/s40959-024-00290-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>CD19 CAR T-cell therapy is a novel anti-cancer treatment that has produced remarkable responses in relapsed or refractory B-cell hematological malignancies. Cytokine Release Syndrome (CRS) is a dysregulated immune response that frequently occurs after CAR T-cell infusion. It can cause cardiac dysfunction and circulatory collapse negatively impacting outcomes and survival. To endure the insults of CRS, patients are typically screened for adequate cardiac reserve before treatment. The relationship between baseline cardiac function by echocardiography and the development of moderate to severe presentations of CRS is unclear.</p><p><strong>Methods: </strong>This study aimed to identify baseline echocardiographic variables that can predict the development of hemodynamically significant CRS (CRS ≥ 2), evaluate their behavior at follow-up, and investigate the incidence of cancer therapy-related cardiac dysfunction (CTRCD). An observational retrospective cohort study of patients treated with CD19 CAR T-cell therapy with a baseline echocardiogram was performed. Demographic, clinical and echocardiographic variables were abstracted from the electronic health record. Patients were grouped and compared by the occurrence of CRS < 2 and ≥ 2. Adjusted logistic regression analysis was used to evaluate the association between echocardiographic variables and the development of CRS ≥ 2.</p><p><strong>Results: </strong>291 patients were included in the study. Median age was 60 (IQR: 51, 67 years), 73% were male, and 71% had diffuse large B-cell lymphoma. Logistic regression analysis did not reveal any significant baseline echocardiographic predictors of CRS ≥ 2, including left ventricular ejection fraction and global longitudinal strain. Systolic and diastolic echocardiographic variables remained within normal limits at follow-up overall and in both CRS groups. The incidence of CTRCD was 4.5% and occurred mostly in the setting of CRS ≥ 2.</p><p><strong>Conclusion: </strong>No specific echocardiographic variables predicted the development of CRS ≥ 2, and therefore the mechanism leading to hemodynamic decompensation and producing worsening hypoxia and hypotension could be multifactorial and not directly cardiac mediated.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"91"},"PeriodicalIF":3.2000,"publicationDate":"2024-12-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11662545/pdf/","citationCount":"0","resultStr":"{\"title\":\"Baseline echocardiographic variables as predictors of hemodynamically significant cytokine release syndrome in adults treated with CD19 CAR T-cell therapy for hematological malignancies.\",\"authors\":\"Andres E Daryanani, Muhannad A Abbasi, Maria F Gomez Ardila, Eduardo Tellez-Garcia, Juan M Garzon-Dangond, Yi Lin, Jonas Paludo, Joerg Herrmann, Stephen M Ansell, Allison C Rosenthal, Hector R Villarraga\",\"doi\":\"10.1186/s40959-024-00290-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>CD19 CAR T-cell therapy is a novel anti-cancer treatment that has produced remarkable responses in relapsed or refractory B-cell hematological malignancies. Cytokine Release Syndrome (CRS) is a dysregulated immune response that frequently occurs after CAR T-cell infusion. It can cause cardiac dysfunction and circulatory collapse negatively impacting outcomes and survival. To endure the insults of CRS, patients are typically screened for adequate cardiac reserve before treatment. The relationship between baseline cardiac function by echocardiography and the development of moderate to severe presentations of CRS is unclear.</p><p><strong>Methods: </strong>This study aimed to identify baseline echocardiographic variables that can predict the development of hemodynamically significant CRS (CRS ≥ 2), evaluate their behavior at follow-up, and investigate the incidence of cancer therapy-related cardiac dysfunction (CTRCD). An observational retrospective cohort study of patients treated with CD19 CAR T-cell therapy with a baseline echocardiogram was performed. Demographic, clinical and echocardiographic variables were abstracted from the electronic health record. Patients were grouped and compared by the occurrence of CRS < 2 and ≥ 2. Adjusted logistic regression analysis was used to evaluate the association between echocardiographic variables and the development of CRS ≥ 2.</p><p><strong>Results: </strong>291 patients were included in the study. Median age was 60 (IQR: 51, 67 years), 73% were male, and 71% had diffuse large B-cell lymphoma. Logistic regression analysis did not reveal any significant baseline echocardiographic predictors of CRS ≥ 2, including left ventricular ejection fraction and global longitudinal strain. Systolic and diastolic echocardiographic variables remained within normal limits at follow-up overall and in both CRS groups. The incidence of CTRCD was 4.5% and occurred mostly in the setting of CRS ≥ 2.</p><p><strong>Conclusion: </strong>No specific echocardiographic variables predicted the development of CRS ≥ 2, and therefore the mechanism leading to hemodynamic decompensation and producing worsening hypoxia and hypotension could be multifactorial and not directly cardiac mediated.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"10 1\",\"pages\":\"91\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-12-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11662545/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-024-00290-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00290-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:CD19 CAR - t细胞疗法是一种新的抗癌疗法,在复发或难治性b细胞恶性血液病中产生了显著的疗效。细胞因子释放综合征(CRS)是一种失调的免疫反应,经常发生在CAR - t细胞输注后。它会导致心功能障碍和循环衰竭,对预后和生存产生负面影响。为了忍受CRS的伤害,患者通常在治疗前进行心脏储备筛查。超声心动图的基线心功能与中重度CRS表现之间的关系尚不清楚。方法:本研究旨在确定可以预测血流动力学显著CRS (CRS≥2)发展的基线超声心动图变量,在随访中评估其行为,并调查癌症治疗相关性心功能障碍(CTRCD)的发生率。一项观察性回顾性队列研究对接受CD19 CAR - t细胞治疗的患者进行了基线超声心动图检查。从电子健康记录中提取人口统计学、临床和超声心动图变量。根据CRS的发生情况对患者进行分组比较。结果:共纳入291例患者。中位年龄60岁(IQR: 51,67岁),73%为男性,71%为弥漫性大b细胞淋巴瘤。Logistic回归分析未发现任何显著的基线超声心动图预测CRS≥2,包括左室射血分数和整体纵向应变。收缩期和舒张期超声心动图变量在总体随访和两组CRS中均保持在正常范围内。CTRCD发生率为4.5%,多发生在CRS≥2的情况下。结论:没有特定的超声心动图变量预测CRS≥2的发展,因此导致血流动力学失代偿和缺氧低血压加重的机制可能是多因素的,而不是心脏直接介导的。
Baseline echocardiographic variables as predictors of hemodynamically significant cytokine release syndrome in adults treated with CD19 CAR T-cell therapy for hematological malignancies.
Background: CD19 CAR T-cell therapy is a novel anti-cancer treatment that has produced remarkable responses in relapsed or refractory B-cell hematological malignancies. Cytokine Release Syndrome (CRS) is a dysregulated immune response that frequently occurs after CAR T-cell infusion. It can cause cardiac dysfunction and circulatory collapse negatively impacting outcomes and survival. To endure the insults of CRS, patients are typically screened for adequate cardiac reserve before treatment. The relationship between baseline cardiac function by echocardiography and the development of moderate to severe presentations of CRS is unclear.
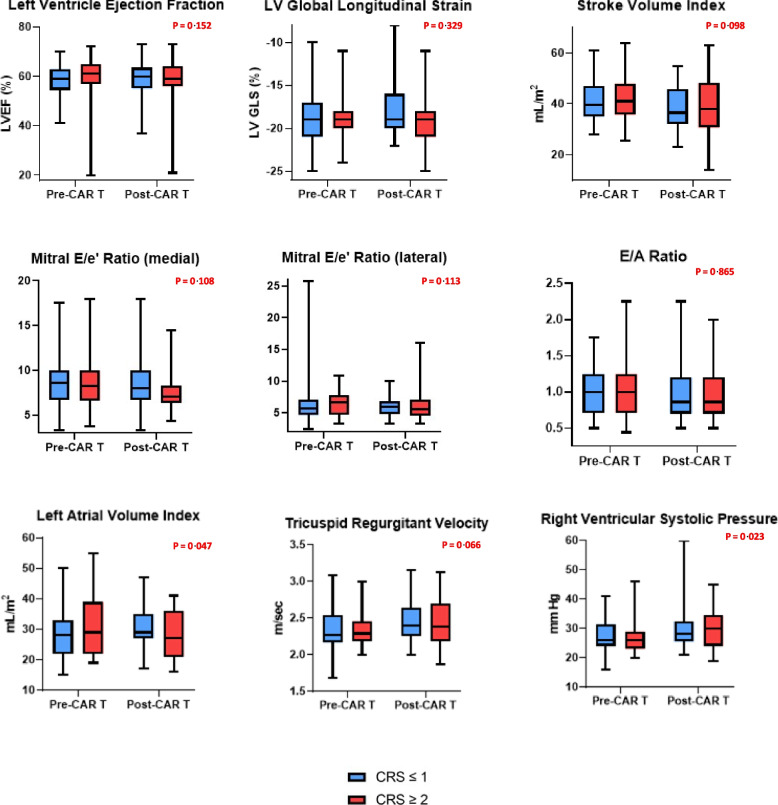
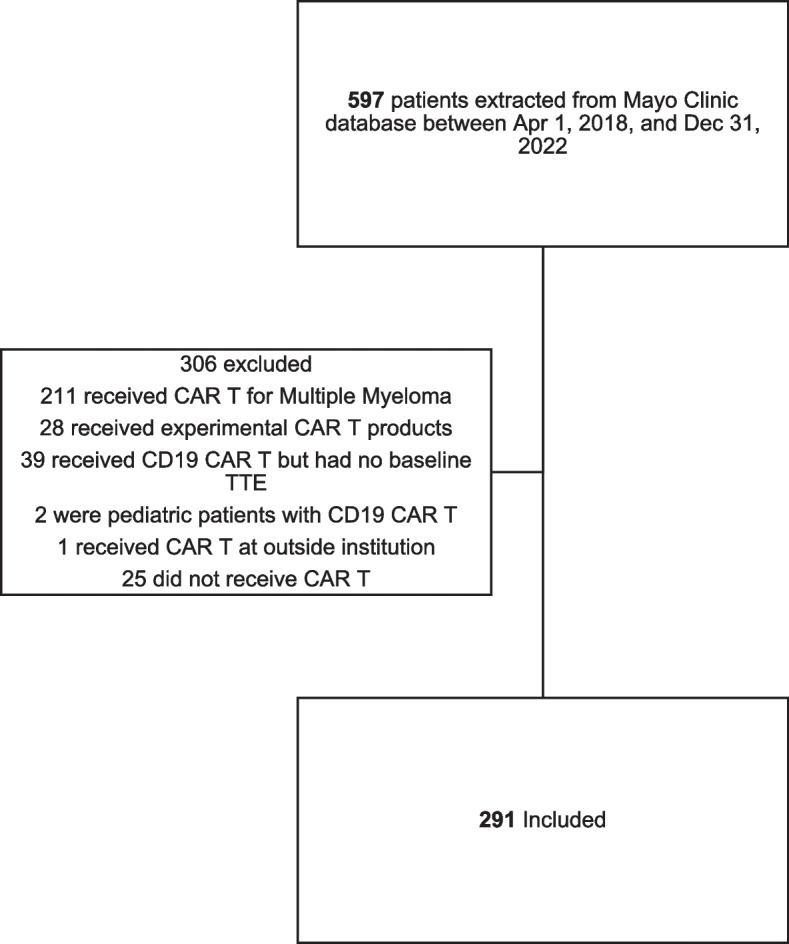
Methods: This study aimed to identify baseline echocardiographic variables that can predict the development of hemodynamically significant CRS (CRS ≥ 2), evaluate their behavior at follow-up, and investigate the incidence of cancer therapy-related cardiac dysfunction (CTRCD). An observational retrospective cohort study of patients treated with CD19 CAR T-cell therapy with a baseline echocardiogram was performed. Demographic, clinical and echocardiographic variables were abstracted from the electronic health record. Patients were grouped and compared by the occurrence of CRS < 2 and ≥ 2. Adjusted logistic regression analysis was used to evaluate the association between echocardiographic variables and the development of CRS ≥ 2.
Results: 291 patients were included in the study. Median age was 60 (IQR: 51, 67 years), 73% were male, and 71% had diffuse large B-cell lymphoma. Logistic regression analysis did not reveal any significant baseline echocardiographic predictors of CRS ≥ 2, including left ventricular ejection fraction and global longitudinal strain. Systolic and diastolic echocardiographic variables remained within normal limits at follow-up overall and in both CRS groups. The incidence of CTRCD was 4.5% and occurred mostly in the setting of CRS ≥ 2.
Conclusion: No specific echocardiographic variables predicted the development of CRS ≥ 2, and therefore the mechanism leading to hemodynamic decompensation and producing worsening hypoxia and hypotension could be multifactorial and not directly cardiac mediated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


