{"title":"肥胖症与多囊卵巢综合症。","authors":"Jin Ju Kim","doi":"10.7570/jomes24035","DOIUrl":null,"url":null,"abstract":"<p><p>The core pathophysiology of polycystic ovary syndrome involves an overproduction of androgens primarily originating from ovarian thecal cells. Two major external triggers promote androgen overproduction in the ovaries: the increased secretion of luteinizing hormone, a consequence of aberrant hypothalamic gonadotropin-releasing hormone secretion dynamics, and compensatory hyperinsulinemia resulting from insulin resistance. Obesity interacts with polycystic ovary syndrome in multiple ways, but a major role of obesity in its pathophysiology is the exacerbation of insulin resistance. Additionally, obesity contributes to polycystic ovary syndrome by facilitating the conversion of precursor hormones to testosterone within adipose cells. Moreover, obesity can lead to relative hyperandrogenemia, which is marked by lower levels of sex hormone binding globulin and increased availability of free testosterone to target tissues. Also, obesity affects the secretion of gonadotropins, resulting in heightened luteinizing hormone secretion or increased sensitivity of thecal cells to luteinizing hormone. Obesity-related insulin resistance might be amplified by alterations in adipokine and inflammatory cytokine production. Ultimately, obesity and polycystic ovary syndrome might share a common genetic predisposition. The cornerstone of managing polycystic ovary syndrome is to address individual symptoms such as hyperandrogenism (hirsutism, acne, and female type boldness), menstrual irregularities, and infertility stemming from anovulation. However, obesity is integral to the pathophysiology of polycystic ovary syndrome and exacerbates all of its features. Therefore, lifestyle modifications aimed at weight reduction should be the primary strategy in overweight or obese women with polycystic ovary syndrome.</p>","PeriodicalId":45386,"journal":{"name":"Journal of Obesity & Metabolic Syndrome","volume":" ","pages":"289-301"},"PeriodicalIF":7.9000,"publicationDate":"2024-12-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704221/pdf/","citationCount":"0","resultStr":"{\"title\":\"Obesity and Polycystic Ovary Syndrome.\",\"authors\":\"Jin Ju Kim\",\"doi\":\"10.7570/jomes24035\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The core pathophysiology of polycystic ovary syndrome involves an overproduction of androgens primarily originating from ovarian thecal cells. Two major external triggers promote androgen overproduction in the ovaries: the increased secretion of luteinizing hormone, a consequence of aberrant hypothalamic gonadotropin-releasing hormone secretion dynamics, and compensatory hyperinsulinemia resulting from insulin resistance. Obesity interacts with polycystic ovary syndrome in multiple ways, but a major role of obesity in its pathophysiology is the exacerbation of insulin resistance. Additionally, obesity contributes to polycystic ovary syndrome by facilitating the conversion of precursor hormones to testosterone within adipose cells. Moreover, obesity can lead to relative hyperandrogenemia, which is marked by lower levels of sex hormone binding globulin and increased availability of free testosterone to target tissues. Also, obesity affects the secretion of gonadotropins, resulting in heightened luteinizing hormone secretion or increased sensitivity of thecal cells to luteinizing hormone. Obesity-related insulin resistance might be amplified by alterations in adipokine and inflammatory cytokine production. Ultimately, obesity and polycystic ovary syndrome might share a common genetic predisposition. The cornerstone of managing polycystic ovary syndrome is to address individual symptoms such as hyperandrogenism (hirsutism, acne, and female type boldness), menstrual irregularities, and infertility stemming from anovulation. However, obesity is integral to the pathophysiology of polycystic ovary syndrome and exacerbates all of its features. Therefore, lifestyle modifications aimed at weight reduction should be the primary strategy in overweight or obese women with polycystic ovary syndrome.</p>\",\"PeriodicalId\":45386,\"journal\":{\"name\":\"Journal of Obesity & Metabolic Syndrome\",\"volume\":\" \",\"pages\":\"289-301\"},\"PeriodicalIF\":7.9000,\"publicationDate\":\"2024-12-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704221/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Obesity & Metabolic Syndrome\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7570/jomes24035\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Obesity & Metabolic Syndrome","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7570/jomes24035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
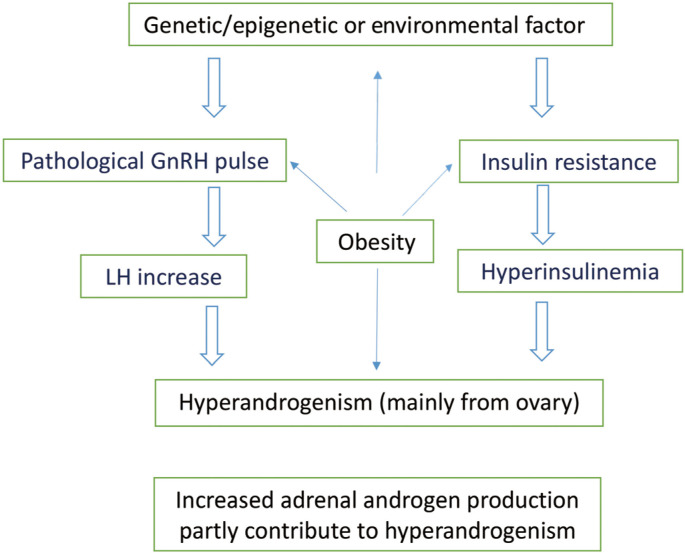
The core pathophysiology of polycystic ovary syndrome involves an overproduction of androgens primarily originating from ovarian thecal cells. Two major external triggers promote androgen overproduction in the ovaries: the increased secretion of luteinizing hormone, a consequence of aberrant hypothalamic gonadotropin-releasing hormone secretion dynamics, and compensatory hyperinsulinemia resulting from insulin resistance. Obesity interacts with polycystic ovary syndrome in multiple ways, but a major role of obesity in its pathophysiology is the exacerbation of insulin resistance. Additionally, obesity contributes to polycystic ovary syndrome by facilitating the conversion of precursor hormones to testosterone within adipose cells. Moreover, obesity can lead to relative hyperandrogenemia, which is marked by lower levels of sex hormone binding globulin and increased availability of free testosterone to target tissues. Also, obesity affects the secretion of gonadotropins, resulting in heightened luteinizing hormone secretion or increased sensitivity of thecal cells to luteinizing hormone. Obesity-related insulin resistance might be amplified by alterations in adipokine and inflammatory cytokine production. Ultimately, obesity and polycystic ovary syndrome might share a common genetic predisposition. The cornerstone of managing polycystic ovary syndrome is to address individual symptoms such as hyperandrogenism (hirsutism, acne, and female type boldness), menstrual irregularities, and infertility stemming from anovulation. However, obesity is integral to the pathophysiology of polycystic ovary syndrome and exacerbates all of its features. Therefore, lifestyle modifications aimed at weight reduction should be the primary strategy in overweight or obese women with polycystic ovary syndrome.
期刊介绍:
The journal was launched in 1992 and diverse studies on obesity have been published under the title of Journal of Korean Society for the Study of Obesity until 2004. Since 2017, volume 26, the title is now the Journal of Obesity & Metabolic Syndrome (pISSN 2508-6235, eISSN 2508-7576). The journal is published quarterly on March 30th, June 30th, September 30th and December 30th. The official title of the journal is now "Journal of Obesity & Metabolic Syndrome" and the abbreviated title is "J Obes Metab Syndr". Index words from medical subject headings (MeSH) list of Index Medicus are included in each article to facilitate article search. Some or all of the articles of this journal are included in the index of PubMed, PubMed Central, Scopus, Embase, DOAJ, Ebsco, KCI, KoreaMed, KoMCI, Science Central, Crossref Metadata Search, Google Scholar, and Emerging Sources Citation Index (ESCI).
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


