不良妊娠结局与认知障碍和痴呆症之间的关系:系统回顾和荟萃分析。
IF 14.6
Q1 GERIATRICS & GERONTOLOGY
引用次数: 0
摘要
背景:不良妊娠结局的个体患脑血管疾病的风险增加,但不良妊娠结局与认知障碍和痴呆之间的关联尚不明确。我们的目的是综合、结合和评估越来越多的数据,这些数据检查了产妇不良妊娠结局与轻度认知障碍和痴呆之间的关系。方法:在这项系统评价和荟萃分析中,我们检索了PubMed (MEDLINE)、Web of Science和Embase数据库,从数据库建立到2024年7月18日,没有语言限制,以观察性研究或临床试验为结果报告轻度认知障碍或痴呆,并纳入了女性个体或有不良妊娠结局的女性,包括妊娠高血压疾病、妊娠糖尿病、死胎、胎儿生长受限、早产、或者胎盘早剥。我们排除了男性、未生育女性、孕前有认知障碍的女性以及怀孕6个月内认知障碍的研究。数据库检索的补充是人工审查纳入研究的参考文献清单。如果研究符合资格标准,但没有足够的数据进行荟萃分析(即,没有报告用于结果估计的汇总统计量或风险比[HR]),则将其纳入系统评价,并从荟萃分析中排除。在删除重复内容后,两名研究人员使用covid - ence软件独立筛选标题和摘要,可能符合条件的研究由同一位审稿人进行全文审查,由第三位审稿人进一步审查,分歧通过讨论和小组共识解决。研究质量由两名评论者独立评估和汇总统计数据。我们研究的主要结局是轻度认知障碍、全因痴呆、阿尔茨海默病和血管性痴呆。采用Q检验和I2统计量来衡量异质性,并使用随机效应模型和反方差加权来评估不良妊娠结局与主要结局之间的相关性,通过合并调整hr和95% ci获得足够的meta分析数据。研究方案已在PROSPERO注册,编号为CRD42023453511。结果:在11 251篇文献中,15篇研究(包括7 347 202名受试者)符合系统评价的纳入标准,11篇研究(6 263 431名受试者)有足够的数据进行meta分析。任何不良妊娠结局的病史与全因痴呆的高风险相关(校正HR 1.32 [95% CI 1.17 - 1.49];I2= 80%),阿尔茨海默病(1.26[1.04 -1·53];I2=63%),血管性痴呆(1.94[1.70 -2·21];I2 = 0%)。妊娠期任何高血压病史与全因痴呆显著相关(1.32 [1.11 - 1.57];I2=74%)和血管性痴呆(1.78 [1.46 ~ 2.17]);I2=0%),但阿尔茨海默病(1.24 [0.98 ~ 1.57];I2 = 66%)。死产与全因痴呆的高风险无显著相关性(1.26 [95% CI 0.93 - 1.71];I2 = 62%)。在个别研究中,早产和胎儿生长受限也观察到类似的影响方向,但数据不足,无法进行meta分析。解释:考虑到她们患痴呆的风险增加,有不良妊娠结局史的妇女应该评估额外的痴呆风险因素,并密切监测任何认知能力下降的迹象。此外,为了获得更可靠的结果,未来的研究应前瞻性和客观地测量暴露和结果。资助:美国国立卫生研究院,美国国立神经疾病和中风研究所,美国国立老龄化研究所,以及美国国立心肺和血液研究所。本文章由计算机程序翻译,如有差异,请以英文原文为准。

Associations between adverse pregnancy outcomes and cognitive impairment and dementia: a systematic review and meta-analysis
Background
Individuals with adverse pregnancy outcomes have an increased risk of cerebrovascular disease, but the association between adverse pregnancy outcomes and cognitive impairment and dementia is less well established. We aimed to synthesise, combine, and assess the growing body of data examining the associations between adverse pregnancy outcomes and mild cognitive impairment and dementia in parous women.
Methods
In this systematic review and meta-analysis, we searched PubMed (MEDLINE), Web of Science, and Embase from database inception up to July 18, 2024, with no language restrictions, for observational studies or clinical trials that reported mild cognitive impairment or dementia as outcomes and included female individuals or women who had an adverse pregnancy outcome, including hypertensive disorders of pregnancy, gestational diabetes, stillbirth, fetal growth restriction, preterm birth, or placental abruption. We excluded studies of men, nulliparous women, women with pre-pregnancy conditions associated with impaired cognition, and studies examining cognitive impairment within 6 months of pregnancy. Database searches were supplemented by manual review of the reference lists of included studies. If studies met eligibility criteria but did not have sufficient data for meta-analysis (ie, did not report a summary statistic or a hazard ratio [HR] for outcome estimation), they were included in the systematic review and excluded from the meta-analysis. After removing duplicates, two investigators independently screened titles and abstracts using Covidence software, with potentially eligible studies undergoing full-text review by the same reviewers, with further review by a third reviewer and disagreements resolved by discussion and group consensus. Study quality was assessed and summary statistics extracted by two reviewers independently. The primary outcomes of our study were mild cognitive impairment, all-cause dementia, Alzheimer’s disease, and vascular dementia. Heterogeneity was measured using the Q test and I2 statistic, and we used random-effects models with inverse-variance weighting to assess the association between adverse pregnancy outcome and primary outcomes with sufficient meta-analysable data via pooled adjusted HRs and 95% CIs. The study protocol was registered with PROSPERO, CRD42023453511.
Findings
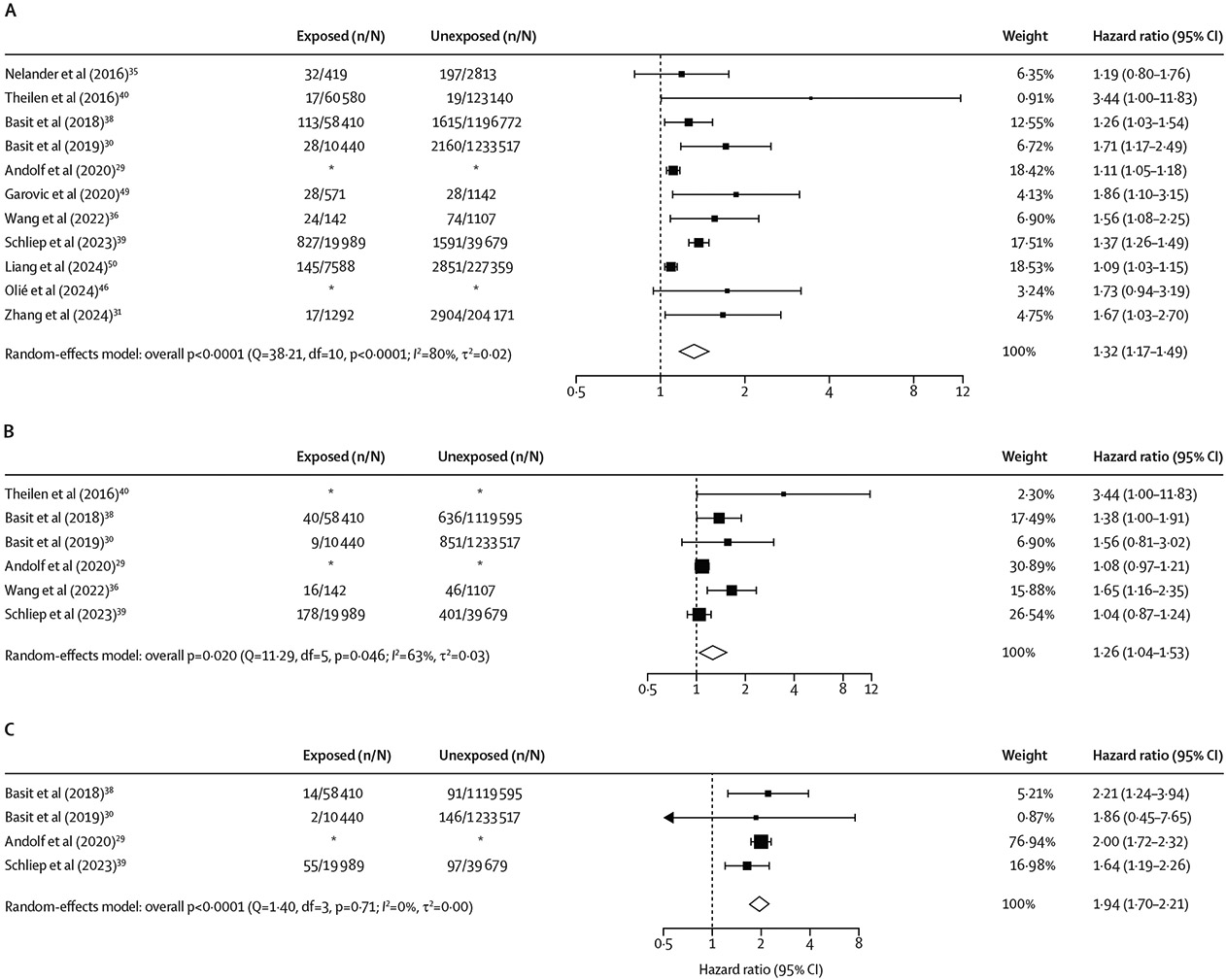
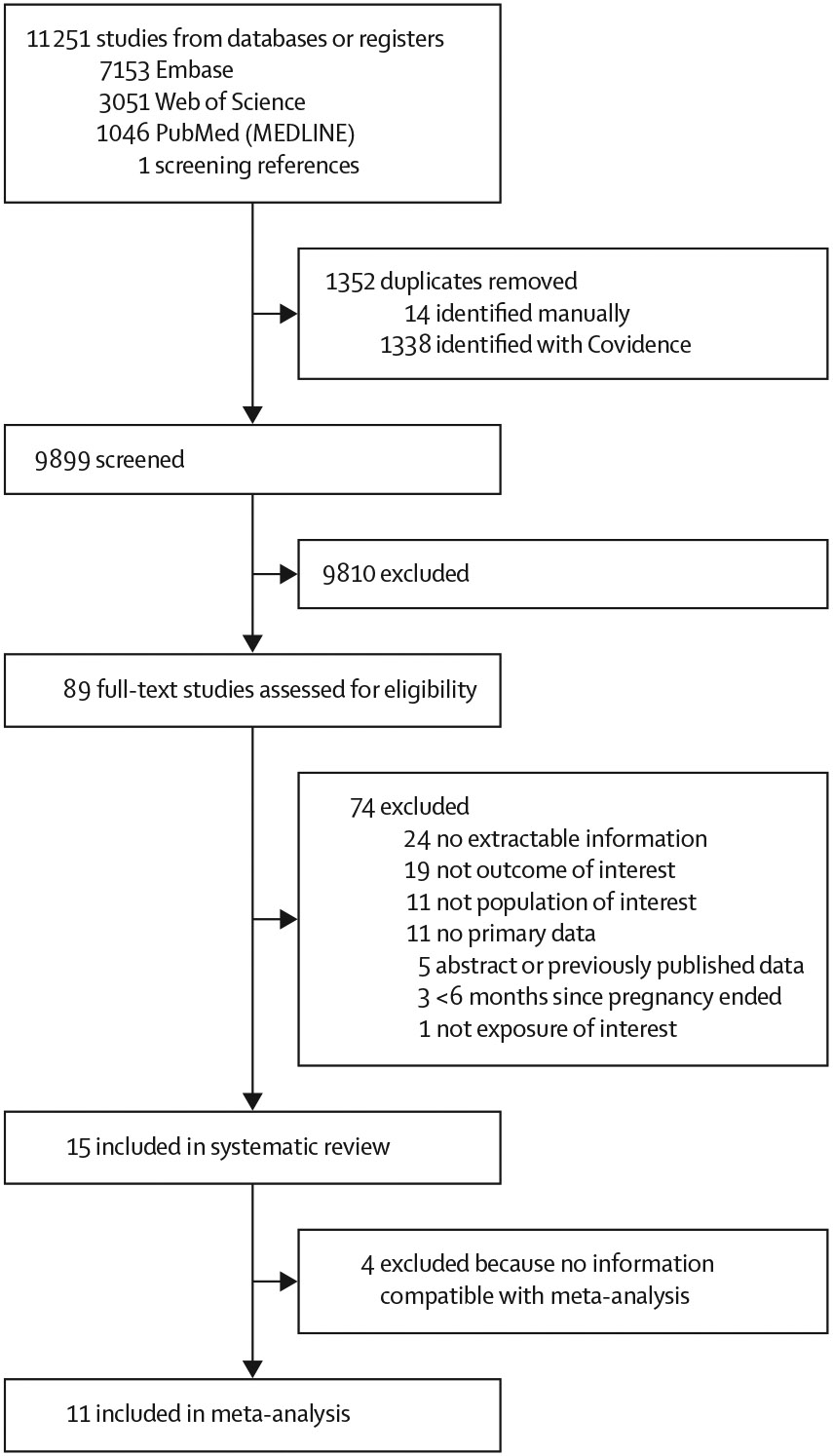
Of 11 251 publications identified, 15 studies (including 7 347 202 participants) met inclusion criteria for the systematic review, and 11 studies (6 263 431 participants) had sufficient data for meta-analysis. A history of any adverse pregnancy outcome was associated with higher risk of all-cause dementia (adjusted HR 1·32 [95% CI 1·17–1·49]; I2= 80%), Alzheimer’s disease (1·26 [1·04–1·53]; I2=63%), and vascular dementia (1·94 [1·70–2·21]; I2=0%). A history of any hypertensive disorder of pregnancy was significantly associated with all-cause dementia (1·32 [1·11–1·57]; I2=74%) and vascular dementia (1·78 [1·46–2·17]; I2=0%), but not Alzheimer’s disease (1·24 [0·98–1·57]; I2=66%). Stillbirth was not significantly associated with higher risk of all-cause dementia (1·26 [95% CI 0·93–1·71]; I2=62%). In individual studies, similar effect directions were observed for preterm birth and fetal growth restriction, but data were insufficient for meta-analysis.
Interpretation
Given their increased risk of dementia, women with a history of adverse pregnancy outcomes should be evaluated for additional dementia risk factors and monitored closely for any signs of cognitive decline. Furthermore, to obtain more reliable findings, future studies should measure both exposures and outcomes prospectively and objectively.
Funding
National Institutes of Health, National Institute of Neurological Disorders and Stroke, National Institute on Aging, and National Heart, Lung and Blood Institute.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Lancet Healthy Longevity
GERIATRICS & GERONTOLOGY-
CiteScore
16.30
自引率
2.30%
发文量
192
审稿时长
12 weeks
期刊介绍:
The Lancet Healthy Longevity, a gold open-access journal, focuses on clinically-relevant longevity and healthy aging research. It covers early-stage clinical research on aging mechanisms, epidemiological studies, and societal research on changing populations. The journal includes clinical trials across disciplines, particularly in gerontology and age-specific clinical guidelines. In line with the Lancet family tradition, it advocates for the rights of all to healthy lives, emphasizing original research likely to impact clinical practice or thinking. Clinical and policy reviews also contribute to shaping the discourse in this rapidly growing discipline.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


