Michael R McClung, Donald Betah, Benjamin Z Leder, David L Kendler, Mary Oates, Jen Timoshanko, Zhenxun Wang
{"title":"罗莫司单抗可改善绝经后骨质疏松症女性的微结构,以组织厚度调整后的骨小梁评分来评估。","authors":"Michael R McClung, Donald Betah, Benjamin Z Leder, David L Kendler, Mary Oates, Jen Timoshanko, Zhenxun Wang","doi":"10.1093/jbmr/zjae194","DOIUrl":null,"url":null,"abstract":"<p><p>Bone mineral density (BMD) is only one of several bone strength determinants affected by osteoporosis therapies. Trabecular Bone Score (TBS), a gray-level texture index determined from lumbar spine (LS) dual-X-ray absorptiometry scans, is an indirect measure of bone microarchitecture independent of and complementary to BMD and clinical risk factors. In the Active-Controlled Fracture Study in Postmenopausal Women with Osteoporosis at High Risk (ARCH), monthly subcutaneous romosozumab 210 mg for 12 mo followed by 24-mo open-label weekly oral alendronate 70 mg (romosozumab-to-alendronate) significantly reduced fracture risk compared to 36-mo alendronate alone in postmenopausal women with osteoporosis and prior fracture. This analysis evaluated tissue thickness-adjusted TBS (TBSTT) in a subgroup of patients from ARCH who had post-hoc TBS measurements at baseline and at least one post-baseline visit at months 12, 24, and 36. Baseline characteristics were similar between romosozumab-to-alendronate (n = 190) and alendronate alone (n = 188). Romosozumab led to significantly greater gains in TBSTT vs alendronate at month 12 (least squares mean difference, 3.6%), with greater gains maintained after transition to alendronate and persisting at months 24 (2.9%) and 36 (2.3%; all p<.001). Romosozumab-to-alendronate increased the percentage of individual patients with \"normal\" TBSTT from 28.9% at baseline to 48.1%, 43.9%, and 45.4% at months 12, 24, and 36, respectively, and decreased the percentage of individual patients with degraded TBSTT from 52.6% to 33.3%, 36.0%, and 33.5%, respectively (all p<.001). A similar but smaller trend was observed with alendronate alone from baseline through month 36 (p ≤.012). Changes in TBSTT and LS BMD were largely unrelated from baseline to month 12 (romosozumab-to-alendronate, r2 = 0.065; alendronate alone, r2 = 0.021) and month 36 (r2 = 0.058; r2 = 0.057, respectively). In postmenopausal women with osteoporosis and prior fracture, 12-mo romosozumab followed by 24-mo alendronate significantly improved bone microarchitecture estimated by TBSTT more than 36-mo alendronate alone.</p>","PeriodicalId":185,"journal":{"name":"Journal of Bone and Mineral Research","volume":" ","pages":"193-200"},"PeriodicalIF":5.9000,"publicationDate":"2025-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11789382/pdf/","citationCount":"0","resultStr":"{\"title\":\"Romosozumab improves microarchitecture as assessed by tissue thickness-adjusted trabecular bone score in postmenopausal women with osteoporosis.\",\"authors\":\"Michael R McClung, Donald Betah, Benjamin Z Leder, David L Kendler, Mary Oates, Jen Timoshanko, Zhenxun Wang\",\"doi\":\"10.1093/jbmr/zjae194\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Bone mineral density (BMD) is only one of several bone strength determinants affected by osteoporosis therapies. Trabecular Bone Score (TBS), a gray-level texture index determined from lumbar spine (LS) dual-X-ray absorptiometry scans, is an indirect measure of bone microarchitecture independent of and complementary to BMD and clinical risk factors. In the Active-Controlled Fracture Study in Postmenopausal Women with Osteoporosis at High Risk (ARCH), monthly subcutaneous romosozumab 210 mg for 12 mo followed by 24-mo open-label weekly oral alendronate 70 mg (romosozumab-to-alendronate) significantly reduced fracture risk compared to 36-mo alendronate alone in postmenopausal women with osteoporosis and prior fracture. This analysis evaluated tissue thickness-adjusted TBS (TBSTT) in a subgroup of patients from ARCH who had post-hoc TBS measurements at baseline and at least one post-baseline visit at months 12, 24, and 36. Baseline characteristics were similar between romosozumab-to-alendronate (n = 190) and alendronate alone (n = 188). Romosozumab led to significantly greater gains in TBSTT vs alendronate at month 12 (least squares mean difference, 3.6%), with greater gains maintained after transition to alendronate and persisting at months 24 (2.9%) and 36 (2.3%; all p<.001). Romosozumab-to-alendronate increased the percentage of individual patients with \\\"normal\\\" TBSTT from 28.9% at baseline to 48.1%, 43.9%, and 45.4% at months 12, 24, and 36, respectively, and decreased the percentage of individual patients with degraded TBSTT from 52.6% to 33.3%, 36.0%, and 33.5%, respectively (all p<.001). A similar but smaller trend was observed with alendronate alone from baseline through month 36 (p ≤.012). Changes in TBSTT and LS BMD were largely unrelated from baseline to month 12 (romosozumab-to-alendronate, r2 = 0.065; alendronate alone, r2 = 0.021) and month 36 (r2 = 0.058; r2 = 0.057, respectively). In postmenopausal women with osteoporosis and prior fracture, 12-mo romosozumab followed by 24-mo alendronate significantly improved bone microarchitecture estimated by TBSTT more than 36-mo alendronate alone.</p>\",\"PeriodicalId\":185,\"journal\":{\"name\":\"Journal of Bone and Mineral Research\",\"volume\":\" \",\"pages\":\"193-200\"},\"PeriodicalIF\":5.9000,\"publicationDate\":\"2025-02-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11789382/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Bone and Mineral Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/jbmr/zjae194\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Mineral Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/jbmr/zjae194","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Romosozumab improves microarchitecture as assessed by tissue thickness-adjusted trabecular bone score in postmenopausal women with osteoporosis.
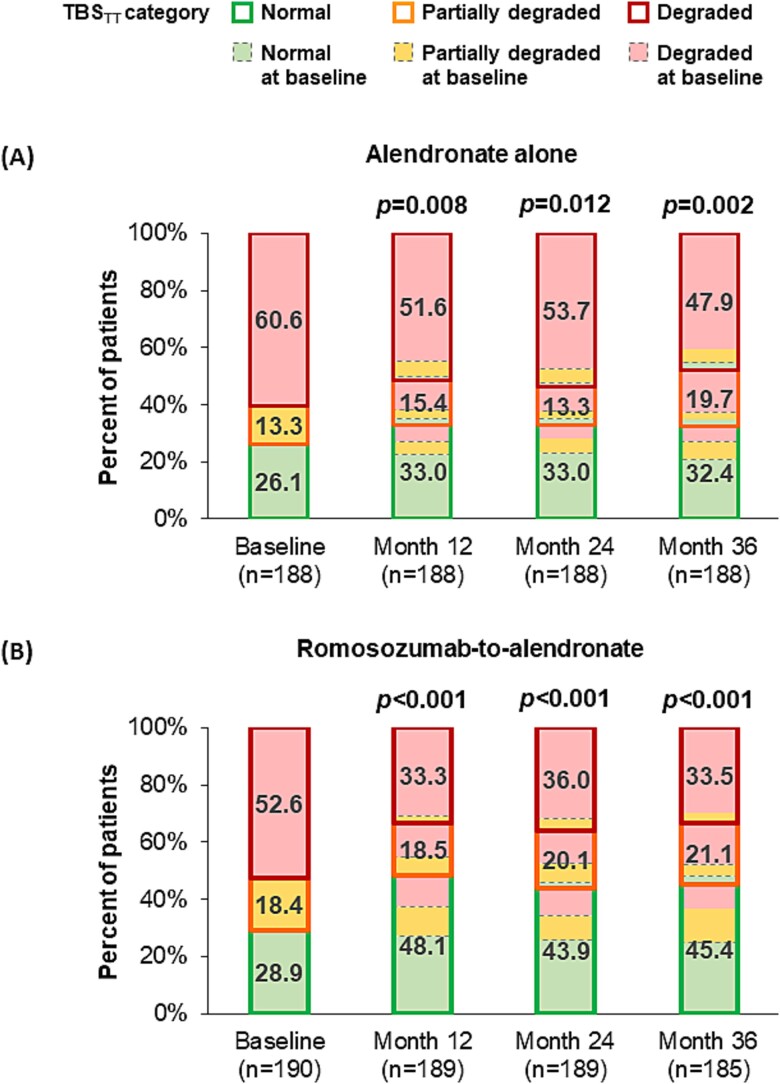
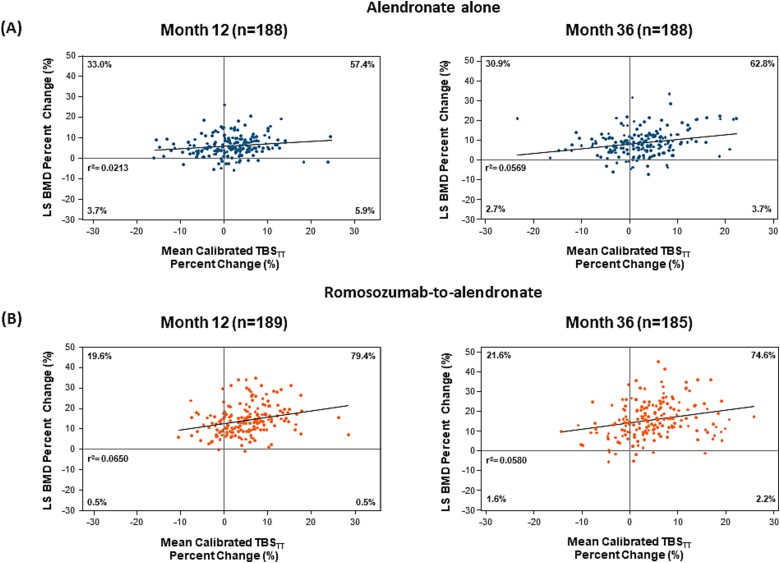
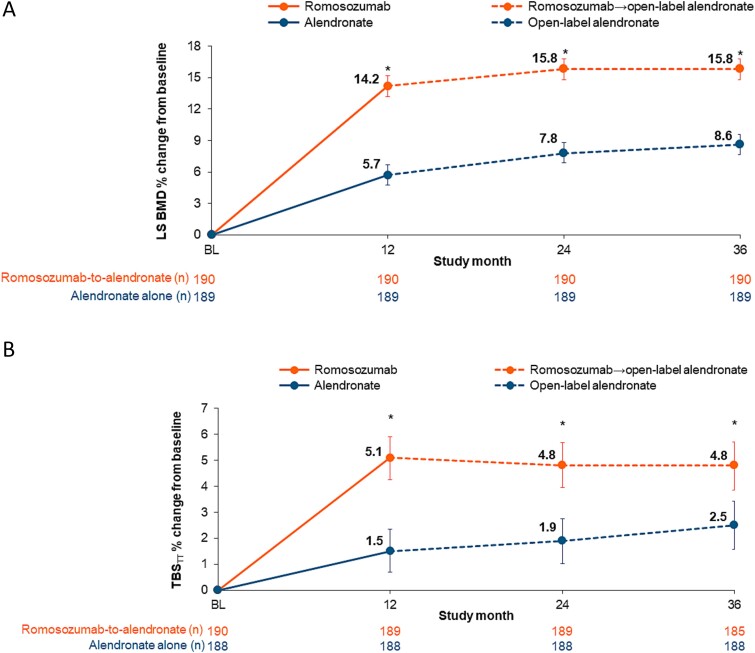
Bone mineral density (BMD) is only one of several bone strength determinants affected by osteoporosis therapies. Trabecular Bone Score (TBS), a gray-level texture index determined from lumbar spine (LS) dual-X-ray absorptiometry scans, is an indirect measure of bone microarchitecture independent of and complementary to BMD and clinical risk factors. In the Active-Controlled Fracture Study in Postmenopausal Women with Osteoporosis at High Risk (ARCH), monthly subcutaneous romosozumab 210 mg for 12 mo followed by 24-mo open-label weekly oral alendronate 70 mg (romosozumab-to-alendronate) significantly reduced fracture risk compared to 36-mo alendronate alone in postmenopausal women with osteoporosis and prior fracture. This analysis evaluated tissue thickness-adjusted TBS (TBSTT) in a subgroup of patients from ARCH who had post-hoc TBS measurements at baseline and at least one post-baseline visit at months 12, 24, and 36. Baseline characteristics were similar between romosozumab-to-alendronate (n = 190) and alendronate alone (n = 188). Romosozumab led to significantly greater gains in TBSTT vs alendronate at month 12 (least squares mean difference, 3.6%), with greater gains maintained after transition to alendronate and persisting at months 24 (2.9%) and 36 (2.3%; all p<.001). Romosozumab-to-alendronate increased the percentage of individual patients with "normal" TBSTT from 28.9% at baseline to 48.1%, 43.9%, and 45.4% at months 12, 24, and 36, respectively, and decreased the percentage of individual patients with degraded TBSTT from 52.6% to 33.3%, 36.0%, and 33.5%, respectively (all p<.001). A similar but smaller trend was observed with alendronate alone from baseline through month 36 (p ≤.012). Changes in TBSTT and LS BMD were largely unrelated from baseline to month 12 (romosozumab-to-alendronate, r2 = 0.065; alendronate alone, r2 = 0.021) and month 36 (r2 = 0.058; r2 = 0.057, respectively). In postmenopausal women with osteoporosis and prior fracture, 12-mo romosozumab followed by 24-mo alendronate significantly improved bone microarchitecture estimated by TBSTT more than 36-mo alendronate alone.
期刊介绍:
The Journal of Bone and Mineral Research (JBMR) publishes highly impactful original manuscripts, reviews, and special articles on basic, translational and clinical investigations relevant to the musculoskeletal system and mineral metabolism. Specifically, the journal is interested in original research on the biology and physiology of skeletal tissues, interdisciplinary research spanning the musculoskeletal and other systems, including but not limited to immunology, hematology, energy metabolism, cancer biology, and neurology, and systems biology topics using large scale “-omics” approaches. The journal welcomes clinical research on the pathophysiology, treatment and prevention of osteoporosis and fractures, as well as sarcopenia, disorders of bone and mineral metabolism, and rare or genetically determined bone diseases.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


