K Dodds, D Curry, P Kelly, D O'Rourke, J McClements
{"title":"目前的做法和结果的患者接受手术切除肾细胞转移到胰腺在北爱尔兰。","authors":"K Dodds, D Curry, P Kelly, D O'Rourke, J McClements","doi":"","DOIUrl":null,"url":null,"abstract":"<p><p>Metastatic tumours to the pancreas are rare but most commonly arise from primary renal cell carcinoma (RCC). Contrary to other metastatic malignancies, metastatic RCC demonstrates indolent behaviour; with a long latency between primary tumour presentation and the development of metastasis, as well as a predilection to isolated pancreas-only disease. As such, pancreatic metastasectomy has evolved as a treatment option for patients with metastatic RCC; reported to associate with improved outcomes in selected patients. The aim of this study was to describe the clinicopathological characteristics and patient outcomes in a series of patients undergoing pancreatic resection for metastatic RCC in a high volume, regional hepatopancreatobiliary (HPB) centre.</p><p><strong>Design: </strong>Retrospective review of all patients who underwent pancreatic metastasectomy for pathologically-confirmed metastatic RCC over an eighteen-year period. Clinicopathological characteristics and outcomes were collected and analysed.</p><p><strong>Results: </strong>Fifteen patients underwent pancreatic resection for metastatic RCC between October 2004 and October 2022. Two patients underwent synchronous nephrectomy and pancreatectomy. In thirteen patients, the pancreas was the only site of metastatic disease. For those with metachronous metastases, the median disease-free interval (DFI) was 126 months from initial nephrectomy.Five-year disease-free and overall survival were 32.7 % and 63.3 %, respectively. No clinicopathological factor was found to associate with overall survival (OS); however, patients with synchronous metastatic disease had a significantly shorter disease-free survival (p = 0.029). Similarly, patients with a longer DFI (≥ ten years) between RCC primary and the development of pancreatic metastases had a trend towards improved OS (p = 0.074).Post-operative morbidity and mortality rates were comparable to that of pancreatic surgery for primary pancreatic pathology.</p><p><strong>Conclusion: </strong>This case series supports the role of pancreatic resection in patients with metastatic RCC, with acceptable rates of morbidity and mortality and favourable patient outcomes. The long DFI between nephrectomy and pancreatic metastases highlights the importance of long-term follow-up for patients diagnosed with RCC.</p>","PeriodicalId":94250,"journal":{"name":"The Ulster medical journal","volume":"93 2","pages":"58-66"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11633314/pdf/","citationCount":"0","resultStr":"{\"title\":\"Current Practice and Outcomes of Patients Undergoing Surgical Resection for Renal Cell Metastases to the Pancreas in Northern Ireland.\",\"authors\":\"K Dodds, D Curry, P Kelly, D O'Rourke, J McClements\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Metastatic tumours to the pancreas are rare but most commonly arise from primary renal cell carcinoma (RCC). Contrary to other metastatic malignancies, metastatic RCC demonstrates indolent behaviour; with a long latency between primary tumour presentation and the development of metastasis, as well as a predilection to isolated pancreas-only disease. As such, pancreatic metastasectomy has evolved as a treatment option for patients with metastatic RCC; reported to associate with improved outcomes in selected patients. The aim of this study was to describe the clinicopathological characteristics and patient outcomes in a series of patients undergoing pancreatic resection for metastatic RCC in a high volume, regional hepatopancreatobiliary (HPB) centre.</p><p><strong>Design: </strong>Retrospective review of all patients who underwent pancreatic metastasectomy for pathologically-confirmed metastatic RCC over an eighteen-year period. Clinicopathological characteristics and outcomes were collected and analysed.</p><p><strong>Results: </strong>Fifteen patients underwent pancreatic resection for metastatic RCC between October 2004 and October 2022. Two patients underwent synchronous nephrectomy and pancreatectomy. In thirteen patients, the pancreas was the only site of metastatic disease. For those with metachronous metastases, the median disease-free interval (DFI) was 126 months from initial nephrectomy.Five-year disease-free and overall survival were 32.7 % and 63.3 %, respectively. No clinicopathological factor was found to associate with overall survival (OS); however, patients with synchronous metastatic disease had a significantly shorter disease-free survival (p = 0.029). Similarly, patients with a longer DFI (≥ ten years) between RCC primary and the development of pancreatic metastases had a trend towards improved OS (p = 0.074).Post-operative morbidity and mortality rates were comparable to that of pancreatic surgery for primary pancreatic pathology.</p><p><strong>Conclusion: </strong>This case series supports the role of pancreatic resection in patients with metastatic RCC, with acceptable rates of morbidity and mortality and favourable patient outcomes. The long DFI between nephrectomy and pancreatic metastases highlights the importance of long-term follow-up for patients diagnosed with RCC.</p>\",\"PeriodicalId\":94250,\"journal\":{\"name\":\"The Ulster medical journal\",\"volume\":\"93 2\",\"pages\":\"58-66\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11633314/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Ulster medical journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Ulster medical journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/11 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Current Practice and Outcomes of Patients Undergoing Surgical Resection for Renal Cell Metastases to the Pancreas in Northern Ireland.
Metastatic tumours to the pancreas are rare but most commonly arise from primary renal cell carcinoma (RCC). Contrary to other metastatic malignancies, metastatic RCC demonstrates indolent behaviour; with a long latency between primary tumour presentation and the development of metastasis, as well as a predilection to isolated pancreas-only disease. As such, pancreatic metastasectomy has evolved as a treatment option for patients with metastatic RCC; reported to associate with improved outcomes in selected patients. The aim of this study was to describe the clinicopathological characteristics and patient outcomes in a series of patients undergoing pancreatic resection for metastatic RCC in a high volume, regional hepatopancreatobiliary (HPB) centre.
Design: Retrospective review of all patients who underwent pancreatic metastasectomy for pathologically-confirmed metastatic RCC over an eighteen-year period. Clinicopathological characteristics and outcomes were collected and analysed.
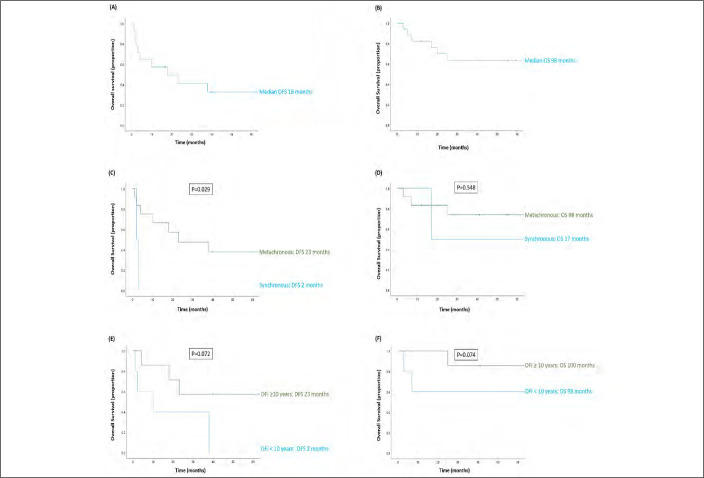
Results: Fifteen patients underwent pancreatic resection for metastatic RCC between October 2004 and October 2022. Two patients underwent synchronous nephrectomy and pancreatectomy. In thirteen patients, the pancreas was the only site of metastatic disease. For those with metachronous metastases, the median disease-free interval (DFI) was 126 months from initial nephrectomy.Five-year disease-free and overall survival were 32.7 % and 63.3 %, respectively. No clinicopathological factor was found to associate with overall survival (OS); however, patients with synchronous metastatic disease had a significantly shorter disease-free survival (p = 0.029). Similarly, patients with a longer DFI (≥ ten years) between RCC primary and the development of pancreatic metastases had a trend towards improved OS (p = 0.074).Post-operative morbidity and mortality rates were comparable to that of pancreatic surgery for primary pancreatic pathology.
Conclusion: This case series supports the role of pancreatic resection in patients with metastatic RCC, with acceptable rates of morbidity and mortality and favourable patient outcomes. The long DFI between nephrectomy and pancreatic metastases highlights the importance of long-term follow-up for patients diagnosed with RCC.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


