Greg Haljan, Terry Lee, Anne McCarthy, Juthaporn Cowan, Jennifer Tsang, Francois Lelouche, Alexis F Turgeon, Patrick Archambault, Francois Lamontagne, Robert Fowler, Jennifer Yoon, Peter Daley, Matthew P Cheng, Donald C Vinh, Todd C Lee, Karen C Tran, Brent W Winston, Hyejin Julia Kong, John H Boyd, Keith R Walley, Allison McGeer, David M Maslove, John C Marshall, Joel Singer, Fagun Jain, James A Russell
{"title":"复杂血栓炎症反应与非COVID-19社区获得性肺炎和COVID-19的结局","authors":"Greg Haljan, Terry Lee, Anne McCarthy, Juthaporn Cowan, Jennifer Tsang, Francois Lelouche, Alexis F Turgeon, Patrick Archambault, Francois Lamontagne, Robert Fowler, Jennifer Yoon, Peter Daley, Matthew P Cheng, Donald C Vinh, Todd C Lee, Karen C Tran, Brent W Winston, Hyejin Julia Kong, John H Boyd, Keith R Walley, Allison McGeer, David M Maslove, John C Marshall, Joel Singer, Fagun Jain, James A Russell","doi":"10.1159/000542420","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The thrombo-inflammatory response and outcomes of community-acquired pneumonia (CAP) due to various organisms (non-COVID-19 CAP) versus CAP due to a single virus, SARS-CoV-2 (i.e., COVID-19) may differ.</p><p><strong>Methods: </strong>Adults hospitalized with non-COVID-19 CAP (December 1, 2021-June 15, 2023) or COVID-19 (March 2, 2020-June 15, 2023) in Canada. We compared non-COVID-19 CAP and COVID-19 baseline, thrombo-inflammatory response, and mortality. We measured plasma cytokine and coagulation factor levels in a sample of patients, did hierarchical clustering, and compared cytokine and coagulation factor levels.</p><p><strong>Results: </strong>In 2,485 patients (non-COVID-19 CAP, n = 719; COVID-19 patients, n = 2,157), non-COVID-19 CAP patients had significantly lower 28-day mortality (CAP vs. COVID-19 waves 1 and 2; 10% vs. 18% and 16%, respectively), intensive care unit admission (CAP vs. all waves; 15% vs. 39%, 37%, 33%, and 24%, respectively), invasive ventilation (CAP vs. waves 1, 2, and 3 patients; 11% vs. 25%, 20%, and 16%), vasopressor use (CAP 12% vs. 23%, 21%, and 18%), and renal replacement therapy use (CAP 3% vs. Omicron 7%). Complexity of hierarchical clustering aligned directly with mortality: COVID-19 wave 1 and 2 patients had six clusters at admission and higher mortality than non-COVID-19 CAP and Omicron that had three clusters at admission. Pooling all COVID-19 waves increased complexity with seven clusters on admission.</p><p><strong>Conclusion: </strong>Complex thrombo-inflammatory responses aligned with mortality of CAP. At a fundamental level, the human thrombo-inflammatory response to a brand new virus was \"confused\" whereas humans had eons of time to develop a more concise efficient thrombo-inflammatory host response to CAP.</p>","PeriodicalId":16113,"journal":{"name":"Journal of Innate Immunity","volume":"16 1","pages":"529-552"},"PeriodicalIF":3.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11614459/pdf/","citationCount":"0","resultStr":"{\"title\":\"Complex Thrombo-Inflammatory Responses versus Outcomes of Non-COVID-19 Community-Acquired Pneumonia and COVID-19.\",\"authors\":\"Greg Haljan, Terry Lee, Anne McCarthy, Juthaporn Cowan, Jennifer Tsang, Francois Lelouche, Alexis F Turgeon, Patrick Archambault, Francois Lamontagne, Robert Fowler, Jennifer Yoon, Peter Daley, Matthew P Cheng, Donald C Vinh, Todd C Lee, Karen C Tran, Brent W Winston, Hyejin Julia Kong, John H Boyd, Keith R Walley, Allison McGeer, David M Maslove, John C Marshall, Joel Singer, Fagun Jain, James A Russell\",\"doi\":\"10.1159/000542420\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The thrombo-inflammatory response and outcomes of community-acquired pneumonia (CAP) due to various organisms (non-COVID-19 CAP) versus CAP due to a single virus, SARS-CoV-2 (i.e., COVID-19) may differ.</p><p><strong>Methods: </strong>Adults hospitalized with non-COVID-19 CAP (December 1, 2021-June 15, 2023) or COVID-19 (March 2, 2020-June 15, 2023) in Canada. We compared non-COVID-19 CAP and COVID-19 baseline, thrombo-inflammatory response, and mortality. We measured plasma cytokine and coagulation factor levels in a sample of patients, did hierarchical clustering, and compared cytokine and coagulation factor levels.</p><p><strong>Results: </strong>In 2,485 patients (non-COVID-19 CAP, n = 719; COVID-19 patients, n = 2,157), non-COVID-19 CAP patients had significantly lower 28-day mortality (CAP vs. COVID-19 waves 1 and 2; 10% vs. 18% and 16%, respectively), intensive care unit admission (CAP vs. all waves; 15% vs. 39%, 37%, 33%, and 24%, respectively), invasive ventilation (CAP vs. waves 1, 2, and 3 patients; 11% vs. 25%, 20%, and 16%), vasopressor use (CAP 12% vs. 23%, 21%, and 18%), and renal replacement therapy use (CAP 3% vs. Omicron 7%). Complexity of hierarchical clustering aligned directly with mortality: COVID-19 wave 1 and 2 patients had six clusters at admission and higher mortality than non-COVID-19 CAP and Omicron that had three clusters at admission. Pooling all COVID-19 waves increased complexity with seven clusters on admission.</p><p><strong>Conclusion: </strong>Complex thrombo-inflammatory responses aligned with mortality of CAP. At a fundamental level, the human thrombo-inflammatory response to a brand new virus was \\\"confused\\\" whereas humans had eons of time to develop a more concise efficient thrombo-inflammatory host response to CAP.</p>\",\"PeriodicalId\":16113,\"journal\":{\"name\":\"Journal of Innate Immunity\",\"volume\":\"16 1\",\"pages\":\"529-552\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11614459/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Innate Immunity\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000542420\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Innate Immunity","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000542420","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
由多种生物(非COVID-19 CAP)引起的社区获得性肺炎(CAP)与由单一病毒SARS-CoV-2(即COVID-19)引起的CAP的血栓炎症反应和结局可能不同。方法:加拿大非COVID-19 CAP(2021年12月1日至2023年6月15日)或COVID-19(2020年3月2日至2023年6月15日)住院的成年人。我们比较了非COVID-19 CAP和COVID-19基线、血栓炎症反应和死亡率。我们在患者样本中测量血浆细胞因子和凝血因子水平,进行分层聚类,并比较细胞因子和凝血因子水平。结果:2485例患者(非covid -19 CAP, n = 719;COVID-19患者,n = 2157),非COVID-19 CAP患者的28天死亡率显著降低(CAP与COVID-19第1波和第2波;10% vs. 18%和16%),重症监护病房入住(CAP vs.所有波浪;分别为15% vs 39%, 37%, 33%和24%),有创通气(CAP vs波1,2和3患者;11%对25%,20%和16%),血管加压药的使用(CAP 12%对23%,21%和18%)和肾脏替代治疗的使用(CAP 3%对Omicron 7%)。分层聚类的复杂性与死亡率直接相关:COVID-19第1波和第2波患者入院时有6个聚类,死亡率高于入院时有3个聚类的非COVID-19 CAP和Omicron。汇集所有COVID-19波增加了复杂性,入院时有七个聚集性病例。结论:复杂的血栓-炎症反应与CAP的死亡率一致。在基本水平上,人类对一种全新病毒的血栓-炎症反应是“混乱的”,而人类有大量的时间来发展一种更简洁有效的血栓-炎症宿主对CAP的反应。
Complex Thrombo-Inflammatory Responses versus Outcomes of Non-COVID-19 Community-Acquired Pneumonia and COVID-19.
Introduction: The thrombo-inflammatory response and outcomes of community-acquired pneumonia (CAP) due to various organisms (non-COVID-19 CAP) versus CAP due to a single virus, SARS-CoV-2 (i.e., COVID-19) may differ.
Methods: Adults hospitalized with non-COVID-19 CAP (December 1, 2021-June 15, 2023) or COVID-19 (March 2, 2020-June 15, 2023) in Canada. We compared non-COVID-19 CAP and COVID-19 baseline, thrombo-inflammatory response, and mortality. We measured plasma cytokine and coagulation factor levels in a sample of patients, did hierarchical clustering, and compared cytokine and coagulation factor levels.
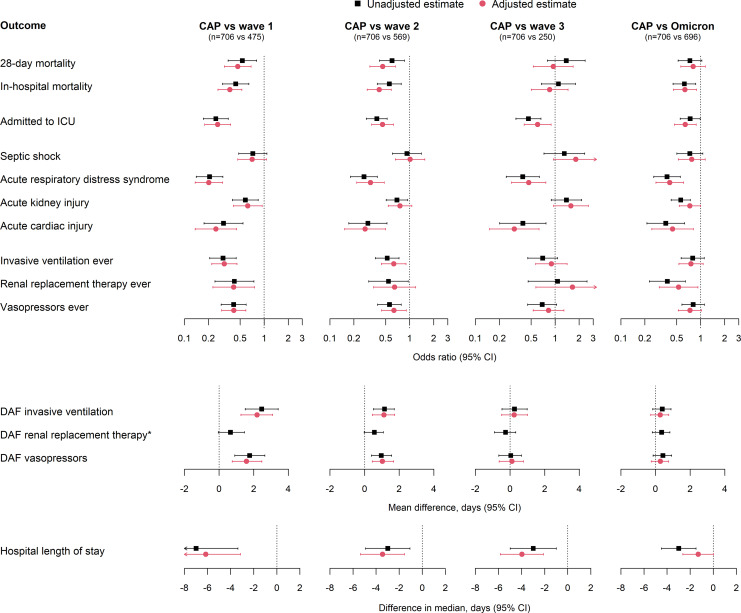
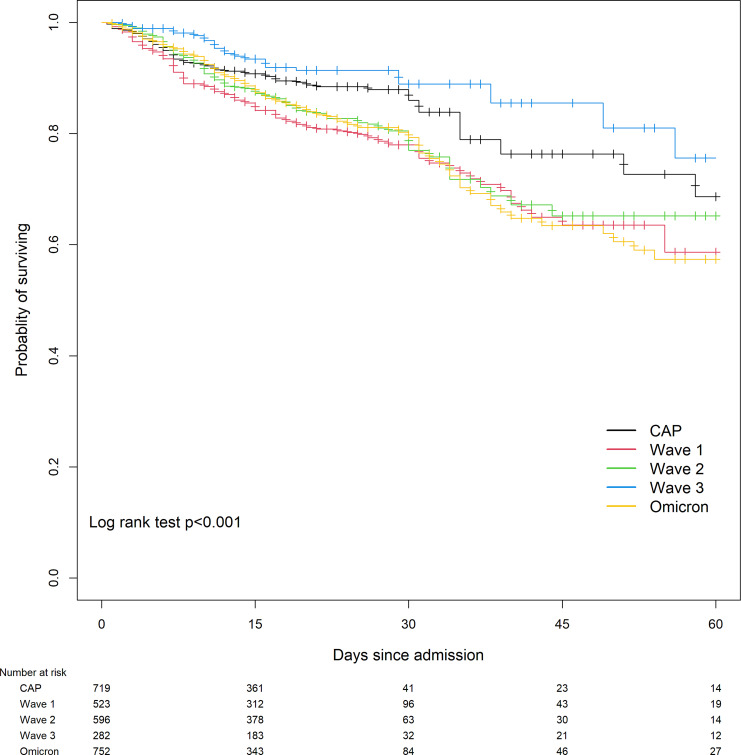
Results: In 2,485 patients (non-COVID-19 CAP, n = 719; COVID-19 patients, n = 2,157), non-COVID-19 CAP patients had significantly lower 28-day mortality (CAP vs. COVID-19 waves 1 and 2; 10% vs. 18% and 16%, respectively), intensive care unit admission (CAP vs. all waves; 15% vs. 39%, 37%, 33%, and 24%, respectively), invasive ventilation (CAP vs. waves 1, 2, and 3 patients; 11% vs. 25%, 20%, and 16%), vasopressor use (CAP 12% vs. 23%, 21%, and 18%), and renal replacement therapy use (CAP 3% vs. Omicron 7%). Complexity of hierarchical clustering aligned directly with mortality: COVID-19 wave 1 and 2 patients had six clusters at admission and higher mortality than non-COVID-19 CAP and Omicron that had three clusters at admission. Pooling all COVID-19 waves increased complexity with seven clusters on admission.
Conclusion: Complex thrombo-inflammatory responses aligned with mortality of CAP. At a fundamental level, the human thrombo-inflammatory response to a brand new virus was "confused" whereas humans had eons of time to develop a more concise efficient thrombo-inflammatory host response to CAP.
期刊介绍:
The ''Journal of Innate Immunity'' is a bimonthly journal covering all aspects within the area of innate immunity, including evolution of the immune system, molecular biology of cells involved in innate immunity, pattern recognition and signals of ‘danger’, microbial corruption, host response and inflammation, mucosal immunity, complement and coagulation, sepsis and septic shock, molecular genomics, and development of immunotherapies. The journal publishes original research articles, short communications, reviews, commentaries and letters to the editors. In addition to regular papers, some issues feature a special section with a thematic focus.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


