{"title":"侵犯左侧阔筋膜肌的深部幼年黄疽:病例报告和文献综述。","authors":"Atsushi Maejima, Keisuke Okuno, Masanori Miyaishi, Daisuke Kawaba, Sosuke Kakee, Kensaku Yamaga, Noriyuki Namba","doi":"10.3960/jslrt.24056","DOIUrl":null,"url":null,"abstract":"<p><p>Juvenile xanthogranuloma (JXG) is a rare benign non-Langerhans cell histiocytosis that usually occurs in cutaneous lesions on the head, neck, or upper trunk of neonates and young children. Intramuscular JXG, which invades muscle tissue, accounts for only 0.6% of all JXGs and mostly occurs in the skeletal muscles of the extremities or trunk. A 5-month-old girl was referred to our hospital. At the age of 3 months, she presented with a slow-growing lump on her left thigh. Magnetic resonance imaging (MRI) showed a 22 × 19 × 18 mm oval mass in her left thigh. First, needle biopsy results suggested deep JXG or myeloid sarcoma. Therefore, marginal resection was performed. Intraoperatively, the tumor adhered to the left tensor fasciae latae muscle and was resected together. Histopathological examination revealed a diffuse monotonous sheet-like proliferation of mononuclear histiocyte-like cells with pale, eosinophilic, foamy cytoplasm with a background of muscle and fatty tissue. Minimal mitotic figures and no nuclear atypia or multinucleated giant cells were observed. Immunohistochemical analysis was positive for CD68 (KP-1) and CD163; weakly positive for lysozyme; and negative for CD1a, S100, myeloperoxidase, and CD34. No blast proliferation was observed in the bone marrow. The patient was diagnosed with deep JXG and scheduled for periodic physical examination and MRI. Despite positive margins, the patient fared well without local recurrence 48 months after tumor removal. Understanding the unique pathology of deep JXG and detailed histological evaluation are important for decision-making.</p>","PeriodicalId":45936,"journal":{"name":"Journal of Clinical and Experimental Hematopathology","volume":" ","pages":"323-327"},"PeriodicalIF":1.4000,"publicationDate":"2024-12-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11786151/pdf/","citationCount":"0","resultStr":"{\"title\":\"Deep juvenile xanthogranuloma invading the left tensor fasciae latae muscle: a case report and a literature review.\",\"authors\":\"Atsushi Maejima, Keisuke Okuno, Masanori Miyaishi, Daisuke Kawaba, Sosuke Kakee, Kensaku Yamaga, Noriyuki Namba\",\"doi\":\"10.3960/jslrt.24056\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Juvenile xanthogranuloma (JXG) is a rare benign non-Langerhans cell histiocytosis that usually occurs in cutaneous lesions on the head, neck, or upper trunk of neonates and young children. Intramuscular JXG, which invades muscle tissue, accounts for only 0.6% of all JXGs and mostly occurs in the skeletal muscles of the extremities or trunk. A 5-month-old girl was referred to our hospital. At the age of 3 months, she presented with a slow-growing lump on her left thigh. Magnetic resonance imaging (MRI) showed a 22 × 19 × 18 mm oval mass in her left thigh. First, needle biopsy results suggested deep JXG or myeloid sarcoma. Therefore, marginal resection was performed. Intraoperatively, the tumor adhered to the left tensor fasciae latae muscle and was resected together. Histopathological examination revealed a diffuse monotonous sheet-like proliferation of mononuclear histiocyte-like cells with pale, eosinophilic, foamy cytoplasm with a background of muscle and fatty tissue. Minimal mitotic figures and no nuclear atypia or multinucleated giant cells were observed. Immunohistochemical analysis was positive for CD68 (KP-1) and CD163; weakly positive for lysozyme; and negative for CD1a, S100, myeloperoxidase, and CD34. No blast proliferation was observed in the bone marrow. The patient was diagnosed with deep JXG and scheduled for periodic physical examination and MRI. Despite positive margins, the patient fared well without local recurrence 48 months after tumor removal. Understanding the unique pathology of deep JXG and detailed histological evaluation are important for decision-making.</p>\",\"PeriodicalId\":45936,\"journal\":{\"name\":\"Journal of Clinical and Experimental Hematopathology\",\"volume\":\" \",\"pages\":\"323-327\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-12-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11786151/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical and Experimental Hematopathology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3960/jslrt.24056\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Experimental Hematopathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3960/jslrt.24056","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/28 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Deep juvenile xanthogranuloma invading the left tensor fasciae latae muscle: a case report and a literature review.
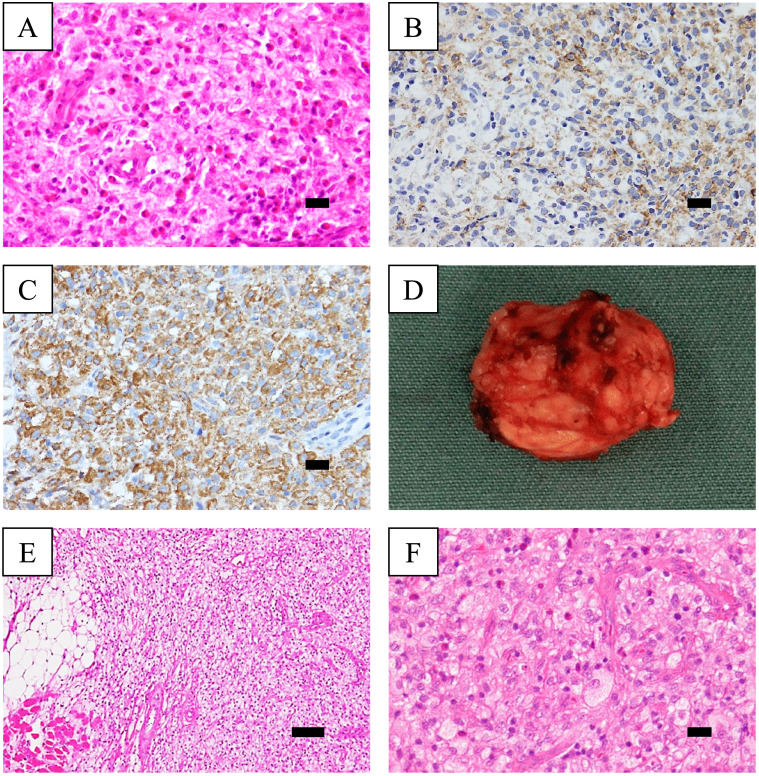
Juvenile xanthogranuloma (JXG) is a rare benign non-Langerhans cell histiocytosis that usually occurs in cutaneous lesions on the head, neck, or upper trunk of neonates and young children. Intramuscular JXG, which invades muscle tissue, accounts for only 0.6% of all JXGs and mostly occurs in the skeletal muscles of the extremities or trunk. A 5-month-old girl was referred to our hospital. At the age of 3 months, she presented with a slow-growing lump on her left thigh. Magnetic resonance imaging (MRI) showed a 22 × 19 × 18 mm oval mass in her left thigh. First, needle biopsy results suggested deep JXG or myeloid sarcoma. Therefore, marginal resection was performed. Intraoperatively, the tumor adhered to the left tensor fasciae latae muscle and was resected together. Histopathological examination revealed a diffuse monotonous sheet-like proliferation of mononuclear histiocyte-like cells with pale, eosinophilic, foamy cytoplasm with a background of muscle and fatty tissue. Minimal mitotic figures and no nuclear atypia or multinucleated giant cells were observed. Immunohistochemical analysis was positive for CD68 (KP-1) and CD163; weakly positive for lysozyme; and negative for CD1a, S100, myeloperoxidase, and CD34. No blast proliferation was observed in the bone marrow. The patient was diagnosed with deep JXG and scheduled for periodic physical examination and MRI. Despite positive margins, the patient fared well without local recurrence 48 months after tumor removal. Understanding the unique pathology of deep JXG and detailed histological evaluation are important for decision-making.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


