{"title":"急性 A 型主动脉夹层的腹内动脉移位与半弓置换策略:一项单中心研究。","authors":"Amarit Phothikun, Nutthayuth Kanokkavinvong, Weerachai Nawarawong, Noppon Taksaudom, Surin Woragidpoonpol","doi":"10.1055/s-0044-1795129","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong> Aggressive surgical methods for acute type A aortic dissection (ATAD) can cause extended operating times and postoperative complications. less extensive techniques may increase the risk of needing further aortic reintervention. To prevent the need for extensive aortic arch surgery and subsequent re-sternotomy, hemiarch replacement (HAR) with innominate artery (a.) translocation is performed to create a suitable proximal landing zone for future endovascular repair.</p><p><strong>Methods: </strong> Retrospective study of 112 patients with ATAD who underwent aortic surgery from January 2009 to December 2020. Forty-one patients underwent HAR with innominate artery translocation, 16 underwent total arch replacement (TAR), and 55 underwent only HAR. Multivariable Cox regression and logistic regression analyses were used to study the outcomes and risk factors.</p><p><strong>Results: </strong> The TAR group had a higher incidence of postoperative acute kidney injury. The overall mortality rate of the TAR group was 25%, compared with 20% in the HAR group and 14.6% in the translocation group. The 5-year overall survival rates for the groups were 81.9%, 75.0%, and 77.7%, respectively. False lumen thrombosis at the aortic arch and descending aorta level were factors associated with reduced mortality in both univariable and multivariable analyses. The translocation group had a significantly higher reintervention rate of 41.5% compared with the TAR and HAR groups, with rates of 31.3% and 16.4%, respectively. The median reintervention time for the translocation group was 4.72 years.</p><p><strong>Conclusion: </strong> Despite the innominate translocation technique having a higher reintervention rate, it had similar mortality outcomes to HAR and TAR. Thus, it could be a more convenient option for reintervention, including creating a proximal landing zone, which could benefit patients needing endovascular repair.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"60-69"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11879489/pdf/","citationCount":"0","resultStr":"{\"title\":\"Innominate Artery Translocation with Hemiarch Replacement Strategy for Acute Type A Aortic Dissection: a Single-Center Study.\",\"authors\":\"Amarit Phothikun, Nutthayuth Kanokkavinvong, Weerachai Nawarawong, Noppon Taksaudom, Surin Woragidpoonpol\",\"doi\":\"10.1055/s-0044-1795129\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong> Aggressive surgical methods for acute type A aortic dissection (ATAD) can cause extended operating times and postoperative complications. less extensive techniques may increase the risk of needing further aortic reintervention. To prevent the need for extensive aortic arch surgery and subsequent re-sternotomy, hemiarch replacement (HAR) with innominate artery (a.) translocation is performed to create a suitable proximal landing zone for future endovascular repair.</p><p><strong>Methods: </strong> Retrospective study of 112 patients with ATAD who underwent aortic surgery from January 2009 to December 2020. Forty-one patients underwent HAR with innominate artery translocation, 16 underwent total arch replacement (TAR), and 55 underwent only HAR. Multivariable Cox regression and logistic regression analyses were used to study the outcomes and risk factors.</p><p><strong>Results: </strong> The TAR group had a higher incidence of postoperative acute kidney injury. The overall mortality rate of the TAR group was 25%, compared with 20% in the HAR group and 14.6% in the translocation group. The 5-year overall survival rates for the groups were 81.9%, 75.0%, and 77.7%, respectively. False lumen thrombosis at the aortic arch and descending aorta level were factors associated with reduced mortality in both univariable and multivariable analyses. The translocation group had a significantly higher reintervention rate of 41.5% compared with the TAR and HAR groups, with rates of 31.3% and 16.4%, respectively. The median reintervention time for the translocation group was 4.72 years.</p><p><strong>Conclusion: </strong> Despite the innominate translocation technique having a higher reintervention rate, it had similar mortality outcomes to HAR and TAR. Thus, it could be a more convenient option for reintervention, including creating a proximal landing zone, which could benefit patients needing endovascular repair.</p>\",\"PeriodicalId\":52392,\"journal\":{\"name\":\"AORTA\",\"volume\":\" \",\"pages\":\"60-69\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11879489/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AORTA\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0044-1795129\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1795129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:针对急性A型主动脉夹层(ATAD)的激进手术方法可能导致手术时间延长和术后并发症。为了避免大面积主动脉弓手术和随后的再梗阻,需要进行半弓置换术(HAR)和腹主动脉(A.)移位术,为将来的血管内修复创造合适的近端着床区:方法:对2009年1月至2020年12月期间接受主动脉手术的112例ATAD患者进行回顾性研究。41名患者接受了带有腹内动脉转位的HAR手术,16名患者接受了全弓置换术(TAR),55名患者仅接受了HAR手术。研究结果和风险因素采用了多变量考克斯回归和逻辑回归分析:结果:TAR组术后急性肾损伤的发生率较高。TAR组的总死亡率为25%,而HAR组为20%,易位组为14.6%。各组的 5 年总生存率分别为 81.9%、75.0% 和 77.7%。在单变量和多变量分析中,主动脉弓和降主动脉水平的假腔血栓是降低死亡率的相关因素。与TAR组和HAR组分别为31.3%和16.4%的再介入率相比,易位组的再介入率明显更高,为41.5%。转位组的再介入时间中位数为 4.72 年:结论:尽管椎弓根转位技术的再介入率较高,但其死亡率与HAR和TAR相似。结论:尽管髂内转位技术的再介入率较高,但其死亡率与 HAR 和 TAR 相似,因此,它可能是一种更方便的再介入选择,包括创建一个近端着床区,这将有利于需要进行血管内修复的患者。
Innominate Artery Translocation with Hemiarch Replacement Strategy for Acute Type A Aortic Dissection: a Single-Center Study.
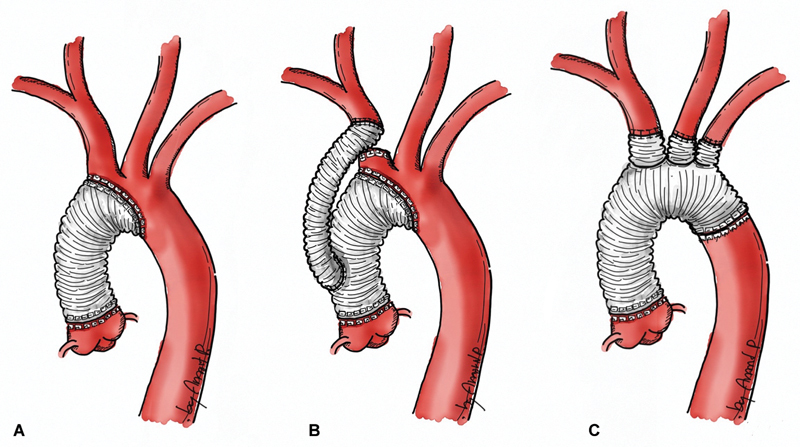
Background: Aggressive surgical methods for acute type A aortic dissection (ATAD) can cause extended operating times and postoperative complications. less extensive techniques may increase the risk of needing further aortic reintervention. To prevent the need for extensive aortic arch surgery and subsequent re-sternotomy, hemiarch replacement (HAR) with innominate artery (a.) translocation is performed to create a suitable proximal landing zone for future endovascular repair.
Methods: Retrospective study of 112 patients with ATAD who underwent aortic surgery from January 2009 to December 2020. Forty-one patients underwent HAR with innominate artery translocation, 16 underwent total arch replacement (TAR), and 55 underwent only HAR. Multivariable Cox regression and logistic regression analyses were used to study the outcomes and risk factors.
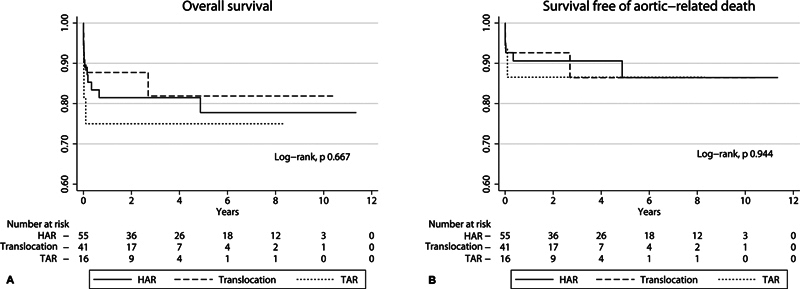
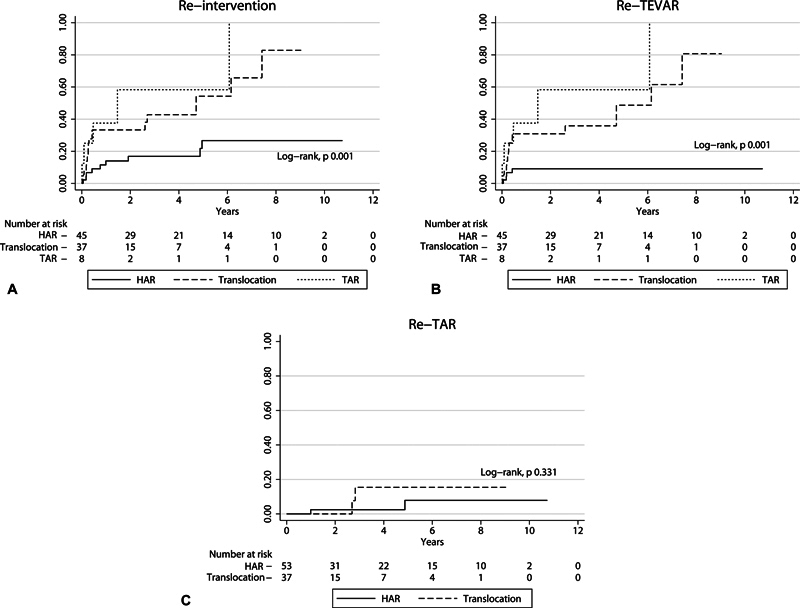
Results: The TAR group had a higher incidence of postoperative acute kidney injury. The overall mortality rate of the TAR group was 25%, compared with 20% in the HAR group and 14.6% in the translocation group. The 5-year overall survival rates for the groups were 81.9%, 75.0%, and 77.7%, respectively. False lumen thrombosis at the aortic arch and descending aorta level were factors associated with reduced mortality in both univariable and multivariable analyses. The translocation group had a significantly higher reintervention rate of 41.5% compared with the TAR and HAR groups, with rates of 31.3% and 16.4%, respectively. The median reintervention time for the translocation group was 4.72 years.
Conclusion: Despite the innominate translocation technique having a higher reintervention rate, it had similar mortality outcomes to HAR and TAR. Thus, it could be a more convenient option for reintervention, including creating a proximal landing zone, which could benefit patients needing endovascular repair.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


