Yutaro Ide, Go Morikawa, Kyohei Yoshida, Yuki Takano, Ken Kubota, Katsuko Okazawa, Takeo Yasu
{"title":"阿司匹林和普拉格雷双重抗血小板疗法期间同时使用质子泵抑制剂与上消化道出血相关的风险:一项回顾性单中心研究。","authors":"Yutaro Ide, Go Morikawa, Kyohei Yoshida, Yuki Takano, Ken Kubota, Katsuko Okazawa, Takeo Yasu","doi":"10.1186/s40780-024-00398-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Dual-antiplatelet therapy (DAPT) and proton pump inhibitor (PPI) are frequently prescribed after percutaneous coronary intervention (PCI) with drug-eluting stents (DES) placement. However, studies that evaluate the optimal PPI when used as primary prevention in patients without a history of peptic ulcer disease or upper gastrointestinal bleeding (UGIB), particularly in the context of DAPT involving prasugrel, are lacking. This study aimed to assess the efficacy and safety of PPI use in preventing UGIB in this patient population.</p><p><strong>Methods: </strong>This study included patients who underwent PCI with coronary stent placement for acute coronary syndrome or stable angina at our institution from January 2015 to December 2020. Eligible patients started DAPT with aspirin and prasugrel and concomitantly received PPI therapy (lansoprazole or esomeprazole), with a follow-up period of two years. The primary endpoint was UGIB incidence, diagnosed during follow-up, serving as an efficacy measure. Secondary endpoints included the assessment of major bleeding (as defined by the Thrombolysis in Myocardial Infarction major bleeding criteria) and clinically relevant non-major bleeding events. Safety outcomes focused on adverse event incidence attributable to PPI use.</p><p><strong>Results: </strong>Among the 165 patients analyzed, 109 and 56 were included in the lansoprazole and esomeprazole groups, respectively, with cumulative incidence of UGIB at 96 weeks of 0.9% (1/109) and 3.6% (2/56). No significant differences in terms of major bleeding events or other bleeding outcomes were observed between the two groups. Adverse events related to PPI use were reported as diarrhea/soft stools in 7 (6%) cases and thrombocytopenia in 1 (1%) case in the lansoprazole group, whereas no such events were observed in the esomeprazole group. No clinically significant hematologic or biochemical abnormalities were reported.</p><p><strong>Conclusion: </strong>This study evaluated the efficacy and safety of PPIs in combination with DAPT, including prasugrel, following PCI, and suggests that lansoprazole and esomeprazole may offer comparable efficacy in preventing UGIB.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"10 1","pages":"76"},"PeriodicalIF":1.2000,"publicationDate":"2024-11-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587642/pdf/","citationCount":"0","resultStr":"{\"title\":\"The risk of upper gastrointestinal bleeding associated with concomitant proton pump inhibitor administration during dual antiplatelet therapy with aspirin and prasugrel: a retrospective single-center study.\",\"authors\":\"Yutaro Ide, Go Morikawa, Kyohei Yoshida, Yuki Takano, Ken Kubota, Katsuko Okazawa, Takeo Yasu\",\"doi\":\"10.1186/s40780-024-00398-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Dual-antiplatelet therapy (DAPT) and proton pump inhibitor (PPI) are frequently prescribed after percutaneous coronary intervention (PCI) with drug-eluting stents (DES) placement. However, studies that evaluate the optimal PPI when used as primary prevention in patients without a history of peptic ulcer disease or upper gastrointestinal bleeding (UGIB), particularly in the context of DAPT involving prasugrel, are lacking. This study aimed to assess the efficacy and safety of PPI use in preventing UGIB in this patient population.</p><p><strong>Methods: </strong>This study included patients who underwent PCI with coronary stent placement for acute coronary syndrome or stable angina at our institution from January 2015 to December 2020. Eligible patients started DAPT with aspirin and prasugrel and concomitantly received PPI therapy (lansoprazole or esomeprazole), with a follow-up period of two years. The primary endpoint was UGIB incidence, diagnosed during follow-up, serving as an efficacy measure. Secondary endpoints included the assessment of major bleeding (as defined by the Thrombolysis in Myocardial Infarction major bleeding criteria) and clinically relevant non-major bleeding events. Safety outcomes focused on adverse event incidence attributable to PPI use.</p><p><strong>Results: </strong>Among the 165 patients analyzed, 109 and 56 were included in the lansoprazole and esomeprazole groups, respectively, with cumulative incidence of UGIB at 96 weeks of 0.9% (1/109) and 3.6% (2/56). No significant differences in terms of major bleeding events or other bleeding outcomes were observed between the two groups. Adverse events related to PPI use were reported as diarrhea/soft stools in 7 (6%) cases and thrombocytopenia in 1 (1%) case in the lansoprazole group, whereas no such events were observed in the esomeprazole group. No clinically significant hematologic or biochemical abnormalities were reported.</p><p><strong>Conclusion: </strong>This study evaluated the efficacy and safety of PPIs in combination with DAPT, including prasugrel, following PCI, and suggests that lansoprazole and esomeprazole may offer comparable efficacy in preventing UGIB.</p>\",\"PeriodicalId\":16730,\"journal\":{\"name\":\"Journal of Pharmaceutical Health Care and Sciences\",\"volume\":\"10 1\",\"pages\":\"76\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-11-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587642/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmaceutical Health Care and Sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40780-024-00398-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-024-00398-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
摘要
目的:使用药物洗脱支架(DES)进行经皮冠状动脉介入治疗(PCI)后,双抗血小板疗法(DAPT)和质子泵抑制剂(PPI)是常用的处方药。然而,目前还缺乏对无消化性溃疡病史或上消化道出血(UGIB)史的患者进行一级预防时使用的最佳 PPI 进行评估的研究,尤其是在使用普拉格雷的 DAPT 时。本研究旨在评估使用 PPI 预防这类患者 UGIB 的有效性和安全性:本研究纳入了2015年1月至2020年12月期间在我院因急性冠脉综合征或稳定型心绞痛接受PCI并植入冠状动脉支架的患者。符合条件的患者开始使用阿司匹林和普拉格雷进行 DAPT,同时接受 PPI 治疗(兰索拉唑或埃索美拉唑),随访期为两年。主要终点是随访期间确诊的 UGIB 发生率,作为疗效衡量标准。次要终点包括评估大出血(根据心肌梗死溶栓治疗大出血标准定义)和临床相关的非大出血事件。安全性结果主要关注使用 PPI 引起的不良事件发生率:在分析的165例患者中,兰索拉唑组和埃索美拉唑组分别有109例和56例患者,96周时UGIB的累计发生率分别为0.9%(1/109)和3.6%(2/56)。两组在大出血事件或其他出血结果方面未发现明显差异。据报告,兰索拉唑组有7例(6%)腹泻/软便,1例(1%)血小板减少,而埃索美拉唑组未观察到与使用PPI相关的不良事件。未报告有临床意义的血液学或生化异常:本研究评估了PCI术后PPIs与包括普拉格雷在内的DAPT联用的疗效和安全性,结果表明兰索拉唑和埃索美拉唑在预防UGIB方面的疗效相当。
The risk of upper gastrointestinal bleeding associated with concomitant proton pump inhibitor administration during dual antiplatelet therapy with aspirin and prasugrel: a retrospective single-center study.
Objective: Dual-antiplatelet therapy (DAPT) and proton pump inhibitor (PPI) are frequently prescribed after percutaneous coronary intervention (PCI) with drug-eluting stents (DES) placement. However, studies that evaluate the optimal PPI when used as primary prevention in patients without a history of peptic ulcer disease or upper gastrointestinal bleeding (UGIB), particularly in the context of DAPT involving prasugrel, are lacking. This study aimed to assess the efficacy and safety of PPI use in preventing UGIB in this patient population.
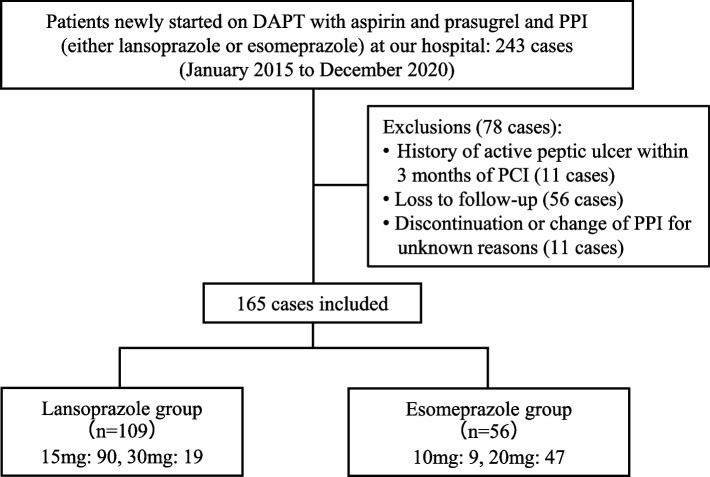
Methods: This study included patients who underwent PCI with coronary stent placement for acute coronary syndrome or stable angina at our institution from January 2015 to December 2020. Eligible patients started DAPT with aspirin and prasugrel and concomitantly received PPI therapy (lansoprazole or esomeprazole), with a follow-up period of two years. The primary endpoint was UGIB incidence, diagnosed during follow-up, serving as an efficacy measure. Secondary endpoints included the assessment of major bleeding (as defined by the Thrombolysis in Myocardial Infarction major bleeding criteria) and clinically relevant non-major bleeding events. Safety outcomes focused on adverse event incidence attributable to PPI use.
Results: Among the 165 patients analyzed, 109 and 56 were included in the lansoprazole and esomeprazole groups, respectively, with cumulative incidence of UGIB at 96 weeks of 0.9% (1/109) and 3.6% (2/56). No significant differences in terms of major bleeding events or other bleeding outcomes were observed between the two groups. Adverse events related to PPI use were reported as diarrhea/soft stools in 7 (6%) cases and thrombocytopenia in 1 (1%) case in the lansoprazole group, whereas no such events were observed in the esomeprazole group. No clinically significant hematologic or biochemical abnormalities were reported.
Conclusion: This study evaluated the efficacy and safety of PPIs in combination with DAPT, including prasugrel, following PCI, and suggests that lansoprazole and esomeprazole may offer comparable efficacy in preventing UGIB.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


