{"title":"股骨颈壁各弯曲表面 X 射线的 C 型臂术中角度调整:一项尸体研究。","authors":"Qiu-Liang Zhu, Xiang-Ping Yu, Jun Ma, Fang Lin, Yun-Yun Chen, Wen-Bin Ruan","doi":"10.1186/s12891-024-08074-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>C-arm fluoroscopy is the main method assisting surgical reduction and internal fixation of the femoral neck, as traditional anteroposterior and lateral fluoroscopy is insufficient for visualizing the irregular anatomical structure of the femoral neck. We analysed the anatomy of the femoral neck to ascertain the optimal position and angle of the C-arm for adequate visualization of the femoral neck during fluoroscopy.</p><p><strong>Methods: </strong>The femoral neck was divided into anterior, posterosuperior and posteroinferior surfaces. These surfaces and the coronal plane of the femur formed the anterior surface coronal angle (ACA), posterosuperior surface coronal angle (PSCA) and posteroinferior surface coronal angle (PICA), respectively. Three angles of 32 dried femoral samples were measured. In the aluminium model, steel wires penetrated the femoral neck wall, whereas, in the wire model, three Kirschner wires penetrated the femoral neck wall. The C-arm was rotated 5° for a 0°-180° fluoroscopic view of each curved surface. Each specimen was imaged, totalling 111 frames. The optimal angle for fluoroscopic imaging of each surface was ascertained, and fluoroscopic features of the Kirschner wire penetrating the femoral neck cortex at three different angles on fluoroscopy and anteroposterior and lateral radiographs were observed.</p><p><strong>Results: </strong>The femoral neck is irregularly shaped and cylindrical, with the anterior surface longer than the posteroinferior surface. The ACA, PSCA and PICA were 31 ± 4.589°, 67.813 ± 5.052° and 168.688 ± 3.206°, respectively. The optimal angles for visualizing the anterior, posterosuperior and posteroinferior surfaces of the steel wire aluminium foil model under fluoroscopy were 30.781 ± 5.464°, 67.969 ± 3.721°, and 167.813 ± 4.319°, respectively. There was no significant difference in the measurements of the corresponding surface coronal angles (P > 0.05). Kirschner wires penetrating the femoral neck wall were difficult to visualize on traditional anteroposterior and lateral films. Increasing the angle to 30°, 70° or 170° for fluoroscopy allowed clear visualization of Kirschner wires penetrating the femoral cortex.</p><p><strong>Conclusion: </strong>Traditional anteroposterior and lateral fluoroscopic views are insufficient for clear visualization of the true structure of the femoral neck. Additionally, increasing the angle to 30°, 70° or 170° for fluoroscopy allows observation of the fracture reduction quality from the anterior surface, posterosuperior surface and posteroinferior surface of the femoral neck and the damage to the corresponding cortical bone caused by internal fixation.</p><p><strong>Level of evidence: </strong>Level II.</p>","PeriodicalId":9189,"journal":{"name":"BMC Musculoskeletal Disorders","volume":"25 1","pages":"956"},"PeriodicalIF":2.4000,"publicationDate":"2024-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11590487/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intraoperative angulation of the C-arm for X-ray of each curved surface of the femoral neck wall: a cadaveric study.\",\"authors\":\"Qiu-Liang Zhu, Xiang-Ping Yu, Jun Ma, Fang Lin, Yun-Yun Chen, Wen-Bin Ruan\",\"doi\":\"10.1186/s12891-024-08074-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>C-arm fluoroscopy is the main method assisting surgical reduction and internal fixation of the femoral neck, as traditional anteroposterior and lateral fluoroscopy is insufficient for visualizing the irregular anatomical structure of the femoral neck. We analysed the anatomy of the femoral neck to ascertain the optimal position and angle of the C-arm for adequate visualization of the femoral neck during fluoroscopy.</p><p><strong>Methods: </strong>The femoral neck was divided into anterior, posterosuperior and posteroinferior surfaces. These surfaces and the coronal plane of the femur formed the anterior surface coronal angle (ACA), posterosuperior surface coronal angle (PSCA) and posteroinferior surface coronal angle (PICA), respectively. Three angles of 32 dried femoral samples were measured. In the aluminium model, steel wires penetrated the femoral neck wall, whereas, in the wire model, three Kirschner wires penetrated the femoral neck wall. The C-arm was rotated 5° for a 0°-180° fluoroscopic view of each curved surface. Each specimen was imaged, totalling 111 frames. The optimal angle for fluoroscopic imaging of each surface was ascertained, and fluoroscopic features of the Kirschner wire penetrating the femoral neck cortex at three different angles on fluoroscopy and anteroposterior and lateral radiographs were observed.</p><p><strong>Results: </strong>The femoral neck is irregularly shaped and cylindrical, with the anterior surface longer than the posteroinferior surface. The ACA, PSCA and PICA were 31 ± 4.589°, 67.813 ± 5.052° and 168.688 ± 3.206°, respectively. The optimal angles for visualizing the anterior, posterosuperior and posteroinferior surfaces of the steel wire aluminium foil model under fluoroscopy were 30.781 ± 5.464°, 67.969 ± 3.721°, and 167.813 ± 4.319°, respectively. There was no significant difference in the measurements of the corresponding surface coronal angles (P > 0.05). Kirschner wires penetrating the femoral neck wall were difficult to visualize on traditional anteroposterior and lateral films. Increasing the angle to 30°, 70° or 170° for fluoroscopy allowed clear visualization of Kirschner wires penetrating the femoral cortex.</p><p><strong>Conclusion: </strong>Traditional anteroposterior and lateral fluoroscopic views are insufficient for clear visualization of the true structure of the femoral neck. Additionally, increasing the angle to 30°, 70° or 170° for fluoroscopy allows observation of the fracture reduction quality from the anterior surface, posterosuperior surface and posteroinferior surface of the femoral neck and the damage to the corresponding cortical bone caused by internal fixation.</p><p><strong>Level of evidence: </strong>Level II.</p>\",\"PeriodicalId\":9189,\"journal\":{\"name\":\"BMC Musculoskeletal Disorders\",\"volume\":\"25 1\",\"pages\":\"956\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-11-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11590487/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Musculoskeletal Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12891-024-08074-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Musculoskeletal Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12891-024-08074-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Intraoperative angulation of the C-arm for X-ray of each curved surface of the femoral neck wall: a cadaveric study.
Background: C-arm fluoroscopy is the main method assisting surgical reduction and internal fixation of the femoral neck, as traditional anteroposterior and lateral fluoroscopy is insufficient for visualizing the irregular anatomical structure of the femoral neck. We analysed the anatomy of the femoral neck to ascertain the optimal position and angle of the C-arm for adequate visualization of the femoral neck during fluoroscopy.
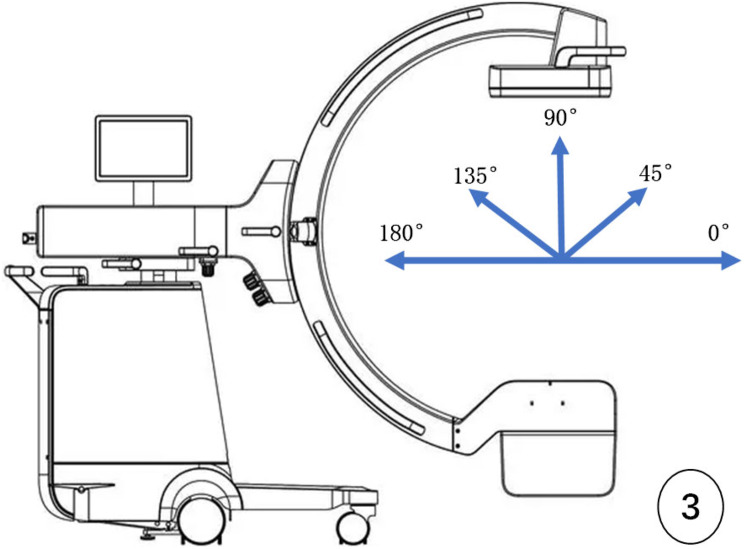
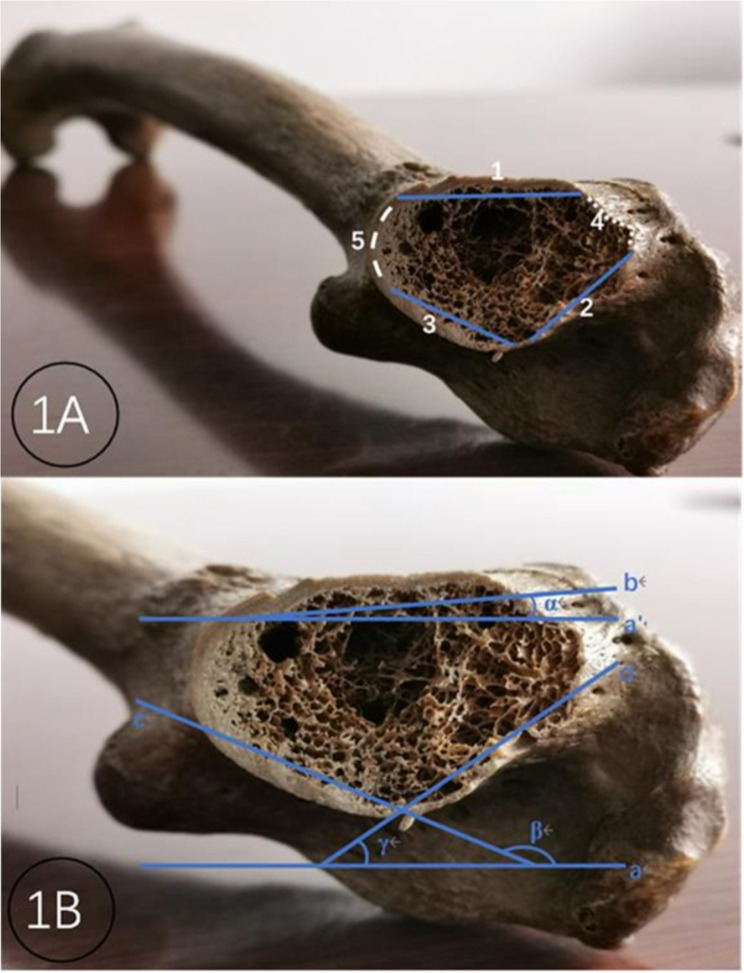
Methods: The femoral neck was divided into anterior, posterosuperior and posteroinferior surfaces. These surfaces and the coronal plane of the femur formed the anterior surface coronal angle (ACA), posterosuperior surface coronal angle (PSCA) and posteroinferior surface coronal angle (PICA), respectively. Three angles of 32 dried femoral samples were measured. In the aluminium model, steel wires penetrated the femoral neck wall, whereas, in the wire model, three Kirschner wires penetrated the femoral neck wall. The C-arm was rotated 5° for a 0°-180° fluoroscopic view of each curved surface. Each specimen was imaged, totalling 111 frames. The optimal angle for fluoroscopic imaging of each surface was ascertained, and fluoroscopic features of the Kirschner wire penetrating the femoral neck cortex at three different angles on fluoroscopy and anteroposterior and lateral radiographs were observed.
Results: The femoral neck is irregularly shaped and cylindrical, with the anterior surface longer than the posteroinferior surface. The ACA, PSCA and PICA were 31 ± 4.589°, 67.813 ± 5.052° and 168.688 ± 3.206°, respectively. The optimal angles for visualizing the anterior, posterosuperior and posteroinferior surfaces of the steel wire aluminium foil model under fluoroscopy were 30.781 ± 5.464°, 67.969 ± 3.721°, and 167.813 ± 4.319°, respectively. There was no significant difference in the measurements of the corresponding surface coronal angles (P > 0.05). Kirschner wires penetrating the femoral neck wall were difficult to visualize on traditional anteroposterior and lateral films. Increasing the angle to 30°, 70° or 170° for fluoroscopy allowed clear visualization of Kirschner wires penetrating the femoral cortex.
Conclusion: Traditional anteroposterior and lateral fluoroscopic views are insufficient for clear visualization of the true structure of the femoral neck. Additionally, increasing the angle to 30°, 70° or 170° for fluoroscopy allows observation of the fracture reduction quality from the anterior surface, posterosuperior surface and posteroinferior surface of the femoral neck and the damage to the corresponding cortical bone caused by internal fixation.
期刊介绍:
BMC Musculoskeletal Disorders is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of musculoskeletal disorders, as well as related molecular genetics, pathophysiology, and epidemiology.
The scope of the Journal covers research into rheumatic diseases where the primary focus relates specifically to a component(s) of the musculoskeletal system.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


