{"title":"钝性外伤性脾损伤患者早期发现延迟性假动脉瘤的随访策略:单中心回顾性研究。","authors":"Sung Hoon Cho, Gun Woo Kim, Suyeong Hwang, Kyoung Hoon Lim","doi":"10.4240/wjgs.v16.i10.3163","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The spleen is the most commonly injured solid organ in blunt abdominal trauma, and splenic pseudoaneurysm rupture is associated with a high risk of mortality. Nonoperative management has become the standard treatment for hemodynamically stable patients with splenic injuries. On the other hand, delayed splenic pseudoaneurysms can develop in any patient, and at present, there are no known risk factors that may reliably predict their occurrence. Furthermore, there is a lack of consensus regarding the most appropriate strategies for monitoring and managing splenic injuries, especially lower-grade (I-III).</p><p><strong>Aim: </strong>To determine the predictors of pseudo-aneurysm formation following splenic injury and develop follow-up strategies for early detection of pseudoaneurysms.</p><p><strong>Methods: </strong>We retrospectively analyzed patients who visited the Level I Trauma Center between January 2013 and December 2022 and were diagnosed with spleen injuries after blunt abdominal trauma.</p><p><strong>Results: </strong>Using the American Association for the Surgery of Trauma spleen injury scale, the splenic injuries were categorized into the following order based on severity: Grade I (<i>n</i> = 57, 17.6%), grade II (<i>n</i> = 114, 35.3%), grade III (<i>n</i> = 89, 27.6%), grade IV (<i>n</i> = 50, 15.5%), and grade V (<i>n</i> = 13, 4.0%). Of a total of 323 patients, 35 underwent splenectomy and 126 underwent angioembolization. 19 underwent delayed angioembolization, and 5 under-went both initial and delayed angioembolization. In 14 patients who had undergone delayed angioembolization, no extravasation or pseudoaneurysm was observed on the initial computed tomography scan. There are no particular patient-related risk factors for the formation of a delayed splenic pseudoaneurysm, which can occur even in a grade I spleen injury or even 21 days after the injury. The mean detection time for a delayed pseudoaneurysm was 6.26 ± 5.4 (1-21, median: 6, interquartile range: 2-9) days.</p><p><strong>Conclusion: </strong>We recommend regular follow-up computed tomography scans, including an arterial and portal venous phase, at least 1 week and 1 month after injury in any grade of blunt traumatic spleen injury for the timely detection of delayed pseudoaneurysms.</p>","PeriodicalId":23759,"journal":{"name":"World Journal of Gastrointestinal Surgery","volume":"16 10","pages":"3163-3170"},"PeriodicalIF":1.7000,"publicationDate":"2024-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11577410/pdf/","citationCount":"0","resultStr":"{\"title\":\"Follow-up strategy for early detection of delayed pseudoaneurysms in patients with blunt traumatic spleen injury: A single-center retrospective study.\",\"authors\":\"Sung Hoon Cho, Gun Woo Kim, Suyeong Hwang, Kyoung Hoon Lim\",\"doi\":\"10.4240/wjgs.v16.i10.3163\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The spleen is the most commonly injured solid organ in blunt abdominal trauma, and splenic pseudoaneurysm rupture is associated with a high risk of mortality. Nonoperative management has become the standard treatment for hemodynamically stable patients with splenic injuries. On the other hand, delayed splenic pseudoaneurysms can develop in any patient, and at present, there are no known risk factors that may reliably predict their occurrence. Furthermore, there is a lack of consensus regarding the most appropriate strategies for monitoring and managing splenic injuries, especially lower-grade (I-III).</p><p><strong>Aim: </strong>To determine the predictors of pseudo-aneurysm formation following splenic injury and develop follow-up strategies for early detection of pseudoaneurysms.</p><p><strong>Methods: </strong>We retrospectively analyzed patients who visited the Level I Trauma Center between January 2013 and December 2022 and were diagnosed with spleen injuries after blunt abdominal trauma.</p><p><strong>Results: </strong>Using the American Association for the Surgery of Trauma spleen injury scale, the splenic injuries were categorized into the following order based on severity: Grade I (<i>n</i> = 57, 17.6%), grade II (<i>n</i> = 114, 35.3%), grade III (<i>n</i> = 89, 27.6%), grade IV (<i>n</i> = 50, 15.5%), and grade V (<i>n</i> = 13, 4.0%). Of a total of 323 patients, 35 underwent splenectomy and 126 underwent angioembolization. 19 underwent delayed angioembolization, and 5 under-went both initial and delayed angioembolization. In 14 patients who had undergone delayed angioembolization, no extravasation or pseudoaneurysm was observed on the initial computed tomography scan. There are no particular patient-related risk factors for the formation of a delayed splenic pseudoaneurysm, which can occur even in a grade I spleen injury or even 21 days after the injury. The mean detection time for a delayed pseudoaneurysm was 6.26 ± 5.4 (1-21, median: 6, interquartile range: 2-9) days.</p><p><strong>Conclusion: </strong>We recommend regular follow-up computed tomography scans, including an arterial and portal venous phase, at least 1 week and 1 month after injury in any grade of blunt traumatic spleen injury for the timely detection of delayed pseudoaneurysms.</p>\",\"PeriodicalId\":23759,\"journal\":{\"name\":\"World Journal of Gastrointestinal Surgery\",\"volume\":\"16 10\",\"pages\":\"3163-3170\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-10-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11577410/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4240/wjgs.v16.i10.3163\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4240/wjgs.v16.i10.3163","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Follow-up strategy for early detection of delayed pseudoaneurysms in patients with blunt traumatic spleen injury: A single-center retrospective study.
Background: The spleen is the most commonly injured solid organ in blunt abdominal trauma, and splenic pseudoaneurysm rupture is associated with a high risk of mortality. Nonoperative management has become the standard treatment for hemodynamically stable patients with splenic injuries. On the other hand, delayed splenic pseudoaneurysms can develop in any patient, and at present, there are no known risk factors that may reliably predict their occurrence. Furthermore, there is a lack of consensus regarding the most appropriate strategies for monitoring and managing splenic injuries, especially lower-grade (I-III).
Aim: To determine the predictors of pseudo-aneurysm formation following splenic injury and develop follow-up strategies for early detection of pseudoaneurysms.
Methods: We retrospectively analyzed patients who visited the Level I Trauma Center between January 2013 and December 2022 and were diagnosed with spleen injuries after blunt abdominal trauma.
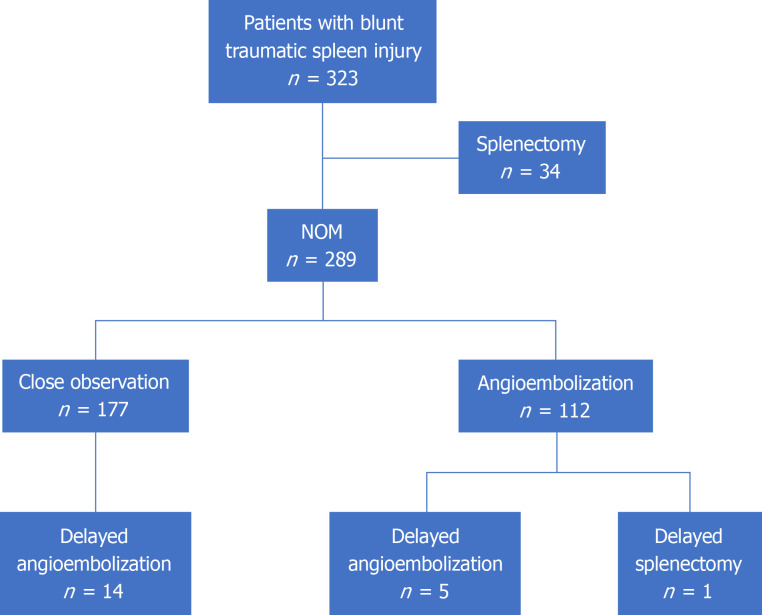
Results: Using the American Association for the Surgery of Trauma spleen injury scale, the splenic injuries were categorized into the following order based on severity: Grade I (n = 57, 17.6%), grade II (n = 114, 35.3%), grade III (n = 89, 27.6%), grade IV (n = 50, 15.5%), and grade V (n = 13, 4.0%). Of a total of 323 patients, 35 underwent splenectomy and 126 underwent angioembolization. 19 underwent delayed angioembolization, and 5 under-went both initial and delayed angioembolization. In 14 patients who had undergone delayed angioembolization, no extravasation or pseudoaneurysm was observed on the initial computed tomography scan. There are no particular patient-related risk factors for the formation of a delayed splenic pseudoaneurysm, which can occur even in a grade I spleen injury or even 21 days after the injury. The mean detection time for a delayed pseudoaneurysm was 6.26 ± 5.4 (1-21, median: 6, interquartile range: 2-9) days.
Conclusion: We recommend regular follow-up computed tomography scans, including an arterial and portal venous phase, at least 1 week and 1 month after injury in any grade of blunt traumatic spleen injury for the timely detection of delayed pseudoaneurysms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


