Caroline Lanz, Jan Meier, Marcel Stöckle, Hansjakob Furrer, Alexandra Calmy, Matthias Cavassini, Enos Bernasconi, Patrick Schmid, Dominique L Braun, Roger D Kouyos, Tom Loosli, Katharina Kusejko, Huldrych F Günthard
{"title":"瑞士艾滋病毒队列研究中,HIV-1 低水平病毒血症可预测接受抗逆转录病毒疗法者的病毒失败。","authors":"Caroline Lanz, Jan Meier, Marcel Stöckle, Hansjakob Furrer, Alexandra Calmy, Matthias Cavassini, Enos Bernasconi, Patrick Schmid, Dominique L Braun, Roger D Kouyos, Tom Loosli, Katharina Kusejko, Huldrych F Günthard","doi":"10.1093/cid/ciae569","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Most individuals receiving combination antiretroviral therapy (ART) have human immunodeficiency virus (HIV) plasma viral loads below the limit of detection. However, episodes of low-level viremia (LLV) are observed in subsets of individuals, the risk factors and clinical significance of which remain debated.</p><p><strong>Methods: </strong>We included participants enrolled in the Swiss HIV Cohort Study, starting ART between July 1999 and April 2023, with HIV RNA values <200 copies/mL 6 months after ART initiation. Using longitudinally collected data, we applied a time-updated Cox proportional hazards model to determine the association of LLV with the risk of subsequent viral failure, defined as ≥200 copies/mL. LLV was quantified by the time-updated area under the curve (AUC) of HIV RNA values, categorized as undetectable or, based on AUC tertiles, low, intermediate, or high.</p><p><strong>Results: </strong>We included 8132 participants with a total of 49 579 person-years of follow-up. The median follow-up time was 4.7 years, and the median number of HIV RNA measurements was 16. Participants had a median age of 38 years, 75.9% were male, 74.4% were white, and 45.9% had HIV-1 subtype B. LLV was associated with an increased risk of subsequent viral failure, with the highest LLV category showing the strongest association (hazard ratio, 3.3 [for comparison with undetectable viral load]) among all included variables, including race/ethnicity, age, and ART.</p><p><strong>Conclusions: </strong>LLV was strongly associated with risk of subsequent viral failure, even after adjustment for demographic and clinical characteristics, including adherence and treatment regimen. The detection of LLV should prompt appropriate measures to decrease the risk of subsequent viral failure.</p>","PeriodicalId":10463,"journal":{"name":"Clinical Infectious Diseases","volume":" ","pages":"57-66"},"PeriodicalIF":7.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314502/pdf/","citationCount":"0","resultStr":"{\"title\":\"HIV-1 Low-Level Viremia Predicts Viral Failure in Participants on Antiretroviral Therapy in the Swiss HIV Cohort Study.\",\"authors\":\"Caroline Lanz, Jan Meier, Marcel Stöckle, Hansjakob Furrer, Alexandra Calmy, Matthias Cavassini, Enos Bernasconi, Patrick Schmid, Dominique L Braun, Roger D Kouyos, Tom Loosli, Katharina Kusejko, Huldrych F Günthard\",\"doi\":\"10.1093/cid/ciae569\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Most individuals receiving combination antiretroviral therapy (ART) have human immunodeficiency virus (HIV) plasma viral loads below the limit of detection. However, episodes of low-level viremia (LLV) are observed in subsets of individuals, the risk factors and clinical significance of which remain debated.</p><p><strong>Methods: </strong>We included participants enrolled in the Swiss HIV Cohort Study, starting ART between July 1999 and April 2023, with HIV RNA values <200 copies/mL 6 months after ART initiation. Using longitudinally collected data, we applied a time-updated Cox proportional hazards model to determine the association of LLV with the risk of subsequent viral failure, defined as ≥200 copies/mL. LLV was quantified by the time-updated area under the curve (AUC) of HIV RNA values, categorized as undetectable or, based on AUC tertiles, low, intermediate, or high.</p><p><strong>Results: </strong>We included 8132 participants with a total of 49 579 person-years of follow-up. The median follow-up time was 4.7 years, and the median number of HIV RNA measurements was 16. Participants had a median age of 38 years, 75.9% were male, 74.4% were white, and 45.9% had HIV-1 subtype B. LLV was associated with an increased risk of subsequent viral failure, with the highest LLV category showing the strongest association (hazard ratio, 3.3 [for comparison with undetectable viral load]) among all included variables, including race/ethnicity, age, and ART.</p><p><strong>Conclusions: </strong>LLV was strongly associated with risk of subsequent viral failure, even after adjustment for demographic and clinical characteristics, including adherence and treatment regimen. The detection of LLV should prompt appropriate measures to decrease the risk of subsequent viral failure.</p>\",\"PeriodicalId\":10463,\"journal\":{\"name\":\"Clinical Infectious Diseases\",\"volume\":\" \",\"pages\":\"57-66\"},\"PeriodicalIF\":7.3000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314502/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Infectious Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/cid/ciae569\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/cid/ciae569","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
HIV-1 Low-Level Viremia Predicts Viral Failure in Participants on Antiretroviral Therapy in the Swiss HIV Cohort Study.
Background: Most individuals receiving combination antiretroviral therapy (ART) have human immunodeficiency virus (HIV) plasma viral loads below the limit of detection. However, episodes of low-level viremia (LLV) are observed in subsets of individuals, the risk factors and clinical significance of which remain debated.
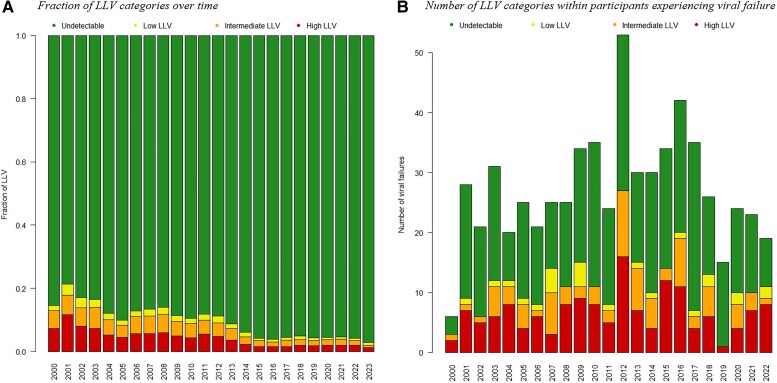
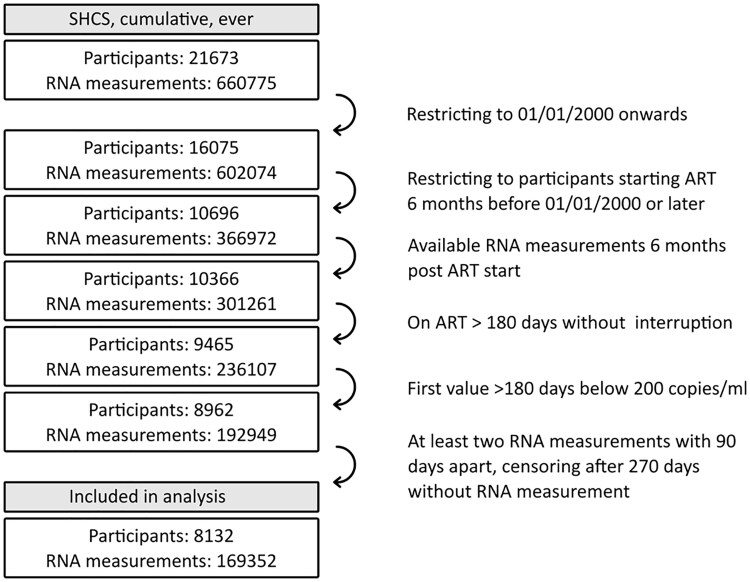
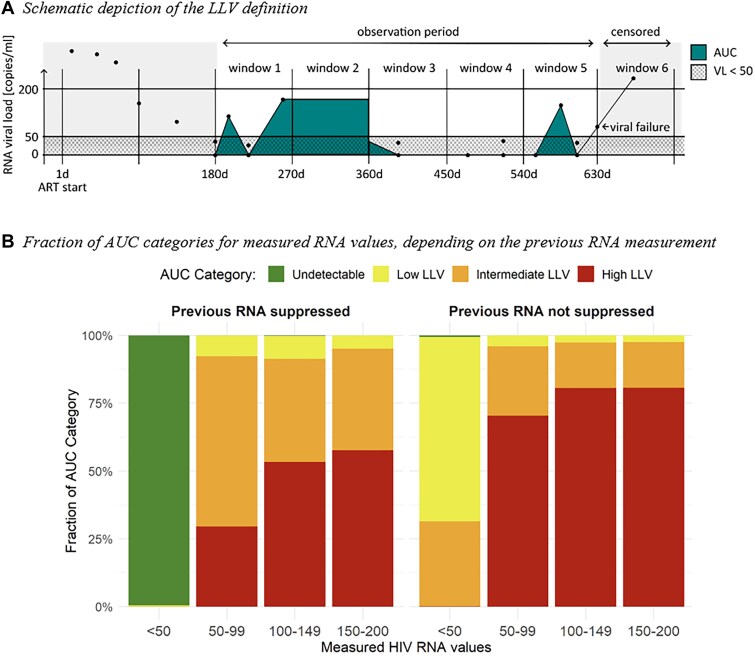
Methods: We included participants enrolled in the Swiss HIV Cohort Study, starting ART between July 1999 and April 2023, with HIV RNA values <200 copies/mL 6 months after ART initiation. Using longitudinally collected data, we applied a time-updated Cox proportional hazards model to determine the association of LLV with the risk of subsequent viral failure, defined as ≥200 copies/mL. LLV was quantified by the time-updated area under the curve (AUC) of HIV RNA values, categorized as undetectable or, based on AUC tertiles, low, intermediate, or high.
Results: We included 8132 participants with a total of 49 579 person-years of follow-up. The median follow-up time was 4.7 years, and the median number of HIV RNA measurements was 16. Participants had a median age of 38 years, 75.9% were male, 74.4% were white, and 45.9% had HIV-1 subtype B. LLV was associated with an increased risk of subsequent viral failure, with the highest LLV category showing the strongest association (hazard ratio, 3.3 [for comparison with undetectable viral load]) among all included variables, including race/ethnicity, age, and ART.
Conclusions: LLV was strongly associated with risk of subsequent viral failure, even after adjustment for demographic and clinical characteristics, including adherence and treatment regimen. The detection of LLV should prompt appropriate measures to decrease the risk of subsequent viral failure.
期刊介绍:
Clinical Infectious Diseases (CID) is dedicated to publishing original research, reviews, guidelines, and perspectives with the potential to reshape clinical practice, providing clinicians with valuable insights for patient care. CID comprehensively addresses the clinical presentation, diagnosis, treatment, and prevention of a wide spectrum of infectious diseases. The journal places a high priority on the assessment of current and innovative treatments, microbiology, immunology, and policies, ensuring relevance to patient care in its commitment to advancing the field of infectious diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


