Ram Ragatha, Ibraheem Khalil, Rebecca Jones, Antonio Manzelli, Alex Reece-Smith, Yunli Ou, Shahjehan Wajed, Davide Di Mauro
{"title":"严重急性结石性胆囊炎患者经皮胆囊造口术后胆结石的临床演变:对 102 例病例的单中心分析。","authors":"Ram Ragatha, Ibraheem Khalil, Rebecca Jones, Antonio Manzelli, Alex Reece-Smith, Yunli Ou, Shahjehan Wajed, Davide Di Mauro","doi":"10.20524/aog.2024.0915","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Percutaneous cholecystostomy (PC) is effective in controlling sepsis in patients with severe acute calculous cholecystitis (ACC). The long-term treatment of this group is still debated. We aimed to assess the clinical evolution of gallstones after severe ACC and the outcomes of laparoscopic cholecystectomy (LC) and conservative management, following PC.</p><p><strong>Methods: </strong>This was a retrospective analysis of the rate of readmissions due to recurrent biliary disease and all-cause mortality in subjects who underwent a PC for severe ACC. We compared results between patients who underwent interval LC and those who received conservative management. Readmissions and late mortality were assessed using the Kaplan-Meier method and multivariate regression analysis.</p><p><strong>Results: </strong>A total of 102 patients were included, of whom 30 underwent interval LC and 72 PC only. Overall, 51.6% were readmitted with recurrent biliary events and the rate did not differ between groups (P=0.583). The probability of recurrent gallstone events was higher in the first 30 weeks after PC; in the surgical cohort, 77.8% of them developed before LC. Late deaths occurred in 46.2% of patients: 13.3% LC vs. 61.9% conservative (P<0.001). Three years after PC, the estimated survival was 75% LC vs. 38% conservative (P=0.014). High-grade comorbidities and severity of ACC were positive predictors of all-cause mortality (P=0.004 and P=0.027), whereas LC was a negative predictor (P=0.003).</p><p><strong>Conclusions: </strong>Recurrent biliary events were common following PC for ACC. Interval LC was associated with lower rates of readmissions and all-cause late mortality.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 6","pages":"718-725"},"PeriodicalIF":2.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574151/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical evolution of gallstones following percutaneous cholecystostomy in patients with severe acute calculous cholecystitis: a single-center analysis of 102 cases.\",\"authors\":\"Ram Ragatha, Ibraheem Khalil, Rebecca Jones, Antonio Manzelli, Alex Reece-Smith, Yunli Ou, Shahjehan Wajed, Davide Di Mauro\",\"doi\":\"10.20524/aog.2024.0915\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Percutaneous cholecystostomy (PC) is effective in controlling sepsis in patients with severe acute calculous cholecystitis (ACC). The long-term treatment of this group is still debated. We aimed to assess the clinical evolution of gallstones after severe ACC and the outcomes of laparoscopic cholecystectomy (LC) and conservative management, following PC.</p><p><strong>Methods: </strong>This was a retrospective analysis of the rate of readmissions due to recurrent biliary disease and all-cause mortality in subjects who underwent a PC for severe ACC. We compared results between patients who underwent interval LC and those who received conservative management. Readmissions and late mortality were assessed using the Kaplan-Meier method and multivariate regression analysis.</p><p><strong>Results: </strong>A total of 102 patients were included, of whom 30 underwent interval LC and 72 PC only. Overall, 51.6% were readmitted with recurrent biliary events and the rate did not differ between groups (P=0.583). The probability of recurrent gallstone events was higher in the first 30 weeks after PC; in the surgical cohort, 77.8% of them developed before LC. Late deaths occurred in 46.2% of patients: 13.3% LC vs. 61.9% conservative (P<0.001). Three years after PC, the estimated survival was 75% LC vs. 38% conservative (P=0.014). High-grade comorbidities and severity of ACC were positive predictors of all-cause mortality (P=0.004 and P=0.027), whereas LC was a negative predictor (P=0.003).</p><p><strong>Conclusions: </strong>Recurrent biliary events were common following PC for ACC. Interval LC was associated with lower rates of readmissions and all-cause late mortality.</p>\",\"PeriodicalId\":7978,\"journal\":{\"name\":\"Annals of Gastroenterology\",\"volume\":\"37 6\",\"pages\":\"718-725\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574151/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20524/aog.2024.0915\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0915","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:经皮胆囊造口术(PC)能有效控制严重急性结石性胆囊炎(ACC)患者的败血症。但对这类患者的长期治疗仍存在争议。我们的目的是评估严重急性结石性胆囊炎后胆结石的临床演变以及PC术后腹腔镜胆囊切除术(LC)和保守治疗的效果:这是一项回顾性分析,研究对象是因重度 ACC 而接受 PC 手术的患者,研究对象因胆道疾病复发而再次入院的比例以及全因死亡率。我们比较了接受间期LC治疗和保守治疗的患者的结果。采用卡普兰-梅耶法和多变量回归分析评估了再住院率和晚期死亡率:结果:共纳入 102 例患者,其中 30 例接受了间歇期 LC 治疗,72 例仅接受 PC 治疗。总体而言,51.6%的患者因复发性胆道事件再次入院,组间比例无差异(P=0.583)。PC术后前30周内复发胆石症的概率较高;在手术组群中,77.8%的患者在LC术前发生胆石症。46.2%的患者在晚期死亡:13.3%的患者在LC术后死亡,61.9%的患者在保守治疗后死亡:ACC PC 术后复发胆道事件很常见。间隔期胆道切除术与较低的再入院率和全因晚期死亡率相关。
Clinical evolution of gallstones following percutaneous cholecystostomy in patients with severe acute calculous cholecystitis: a single-center analysis of 102 cases.
Background: Percutaneous cholecystostomy (PC) is effective in controlling sepsis in patients with severe acute calculous cholecystitis (ACC). The long-term treatment of this group is still debated. We aimed to assess the clinical evolution of gallstones after severe ACC and the outcomes of laparoscopic cholecystectomy (LC) and conservative management, following PC.
Methods: This was a retrospective analysis of the rate of readmissions due to recurrent biliary disease and all-cause mortality in subjects who underwent a PC for severe ACC. We compared results between patients who underwent interval LC and those who received conservative management. Readmissions and late mortality were assessed using the Kaplan-Meier method and multivariate regression analysis.
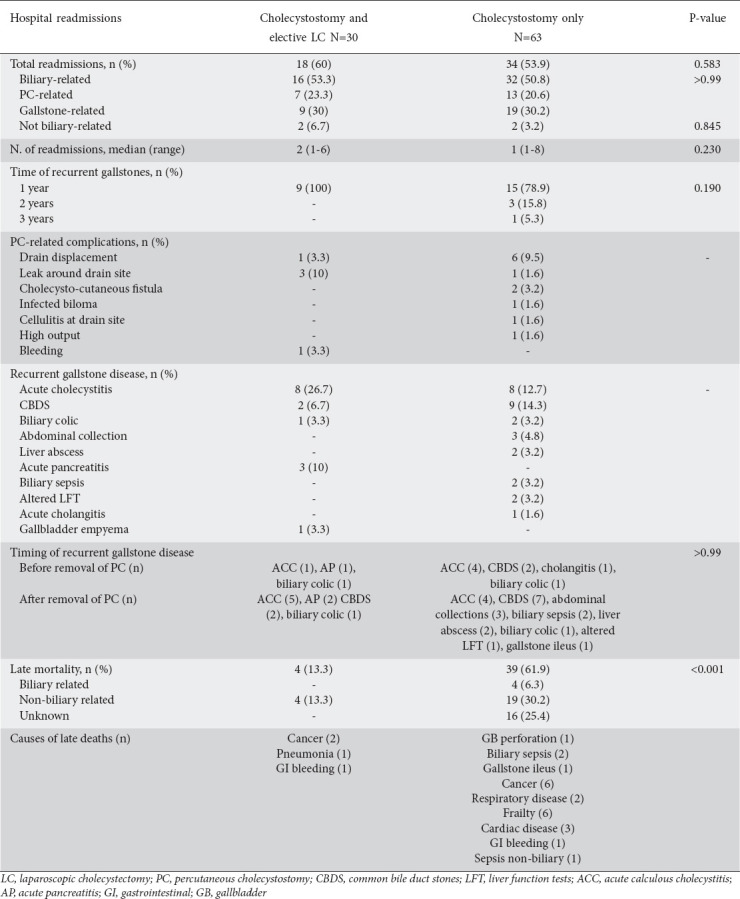
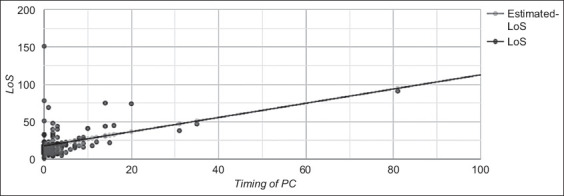
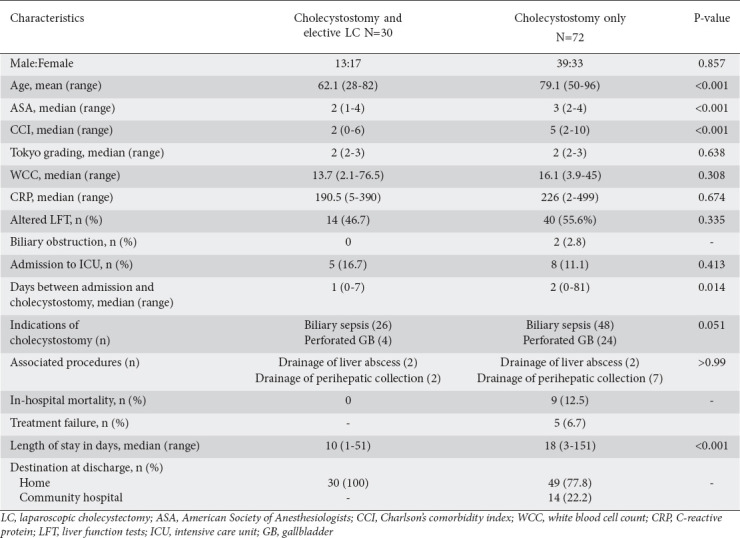
Results: A total of 102 patients were included, of whom 30 underwent interval LC and 72 PC only. Overall, 51.6% were readmitted with recurrent biliary events and the rate did not differ between groups (P=0.583). The probability of recurrent gallstone events was higher in the first 30 weeks after PC; in the surgical cohort, 77.8% of them developed before LC. Late deaths occurred in 46.2% of patients: 13.3% LC vs. 61.9% conservative (P<0.001). Three years after PC, the estimated survival was 75% LC vs. 38% conservative (P=0.014). High-grade comorbidities and severity of ACC were positive predictors of all-cause mortality (P=0.004 and P=0.027), whereas LC was a negative predictor (P=0.003).
Conclusions: Recurrent biliary events were common following PC for ACC. Interval LC was associated with lower rates of readmissions and all-cause late mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


