{"title":"直肠粘膜脱垂综合征(RMPS)的内窥镜特征:与恶性直肠肿瘤的鉴别。","authors":"Yongle Huang, Xiaoqing Lin, Chaoqun Han, Minhu Chen, Zhen Ding","doi":"10.1055/a-2390-2946","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and study aims</b> Rectal mucosal prolapse syndrome (RMPS) usually manifests as rectal bleeding and tenesmus. Endoscopically it can be easily misdiagnosed as malignant rectal tumor (MRT). This study aimed to investigate factors to distinguish RMPS and MRT and to explore endoscopic features of RMPS. <b>Patients and methods</b> Data from patients endoscopically diagnosed with rectal lesions, masses, or tumors, were retrospectively collected. Clinical information, endoscopic images, and histologic reports were reviewed. Patients endoscopically and histologically diagnosed with RMPS were included for phenotype classification. <b>Results</b> 826 patients were enrolled, among them 755 (91.4%), 22 (2.7%), 10 (1.2%), and 39 (4.7%) were respectively diagnosed with MRT, RMPS, endometriosis, and neuroendocrine tumors. Compared with MRT, patients with RMPS were significantly younger (33.5 vs. 62, <i>P</i> < 0.001) and lesions were significantly smaller (2 cm vs. 3 cm, <i>P</i> = 0.007). Moreover, the clinical course of patients with RMPS was significantly longer than for those with MRT (12 months vs. 3 months, <i>P</i> < 0.001). Morphologically, we classified lesions of RMPS into five phenotypes, that is, lesions with circumferential stenosis (19.4%), protrusions (41.7%), both ulcers and protrusions (11.1%), ulcers (11.1%), and flat manifestations (16.7%). Protruding lesions were more frequently observed in females ( <i>P</i> = 0.039), whereas ulcerative lesions were found involving a smaller proportion of the rectal circumference ( <i>P</i> = 0.028). Lesions with only ulcers were found with a shorter distance compared with those with only protrusions (5 cm vs. 10 cm, <i>P</i> = 0.034). <b>Conclusions</b> Age, clinical course, and size of the lesion can be applied to distinguish MRT and RMPS. Five phenotypes have been identified and features of ulcers/protrusions should be further explored.</p>","PeriodicalId":11671,"journal":{"name":"Endoscopy International Open","volume":"12 11","pages":"E1303-E1308"},"PeriodicalIF":2.3000,"publicationDate":"2024-11-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11573464/pdf/","citationCount":"0","resultStr":"{\"title\":\"Endoscopic features of rectal mucosal prolapse syndrome (RMPS): Differentiation from malignant rectal tumor.\",\"authors\":\"Yongle Huang, Xiaoqing Lin, Chaoqun Han, Minhu Chen, Zhen Ding\",\"doi\":\"10.1055/a-2390-2946\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background and study aims</b> Rectal mucosal prolapse syndrome (RMPS) usually manifests as rectal bleeding and tenesmus. Endoscopically it can be easily misdiagnosed as malignant rectal tumor (MRT). This study aimed to investigate factors to distinguish RMPS and MRT and to explore endoscopic features of RMPS. <b>Patients and methods</b> Data from patients endoscopically diagnosed with rectal lesions, masses, or tumors, were retrospectively collected. Clinical information, endoscopic images, and histologic reports were reviewed. Patients endoscopically and histologically diagnosed with RMPS were included for phenotype classification. <b>Results</b> 826 patients were enrolled, among them 755 (91.4%), 22 (2.7%), 10 (1.2%), and 39 (4.7%) were respectively diagnosed with MRT, RMPS, endometriosis, and neuroendocrine tumors. Compared with MRT, patients with RMPS were significantly younger (33.5 vs. 62, <i>P</i> < 0.001) and lesions were significantly smaller (2 cm vs. 3 cm, <i>P</i> = 0.007). Moreover, the clinical course of patients with RMPS was significantly longer than for those with MRT (12 months vs. 3 months, <i>P</i> < 0.001). Morphologically, we classified lesions of RMPS into five phenotypes, that is, lesions with circumferential stenosis (19.4%), protrusions (41.7%), both ulcers and protrusions (11.1%), ulcers (11.1%), and flat manifestations (16.7%). Protruding lesions were more frequently observed in females ( <i>P</i> = 0.039), whereas ulcerative lesions were found involving a smaller proportion of the rectal circumference ( <i>P</i> = 0.028). Lesions with only ulcers were found with a shorter distance compared with those with only protrusions (5 cm vs. 10 cm, <i>P</i> = 0.034). <b>Conclusions</b> Age, clinical course, and size of the lesion can be applied to distinguish MRT and RMPS. Five phenotypes have been identified and features of ulcers/protrusions should be further explored.</p>\",\"PeriodicalId\":11671,\"journal\":{\"name\":\"Endoscopy International Open\",\"volume\":\"12 11\",\"pages\":\"E1303-E1308\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-11-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11573464/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endoscopy International Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2390-2946\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endoscopy International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2390-2946","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Endoscopic features of rectal mucosal prolapse syndrome (RMPS): Differentiation from malignant rectal tumor.
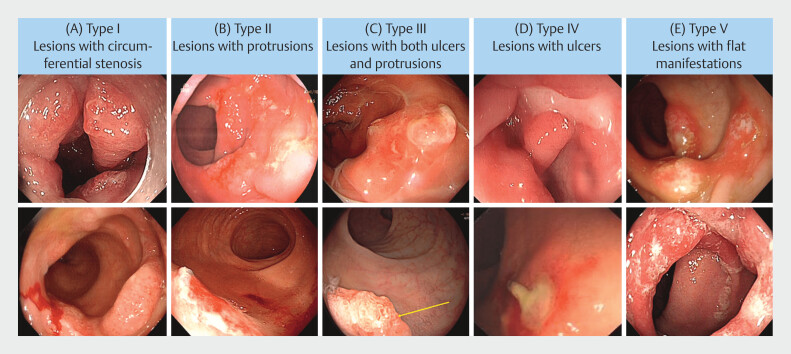
Background and study aims Rectal mucosal prolapse syndrome (RMPS) usually manifests as rectal bleeding and tenesmus. Endoscopically it can be easily misdiagnosed as malignant rectal tumor (MRT). This study aimed to investigate factors to distinguish RMPS and MRT and to explore endoscopic features of RMPS. Patients and methods Data from patients endoscopically diagnosed with rectal lesions, masses, or tumors, were retrospectively collected. Clinical information, endoscopic images, and histologic reports were reviewed. Patients endoscopically and histologically diagnosed with RMPS were included for phenotype classification. Results 826 patients were enrolled, among them 755 (91.4%), 22 (2.7%), 10 (1.2%), and 39 (4.7%) were respectively diagnosed with MRT, RMPS, endometriosis, and neuroendocrine tumors. Compared with MRT, patients with RMPS were significantly younger (33.5 vs. 62, P < 0.001) and lesions were significantly smaller (2 cm vs. 3 cm, P = 0.007). Moreover, the clinical course of patients with RMPS was significantly longer than for those with MRT (12 months vs. 3 months, P < 0.001). Morphologically, we classified lesions of RMPS into five phenotypes, that is, lesions with circumferential stenosis (19.4%), protrusions (41.7%), both ulcers and protrusions (11.1%), ulcers (11.1%), and flat manifestations (16.7%). Protruding lesions were more frequently observed in females ( P = 0.039), whereas ulcerative lesions were found involving a smaller proportion of the rectal circumference ( P = 0.028). Lesions with only ulcers were found with a shorter distance compared with those with only protrusions (5 cm vs. 10 cm, P = 0.034). Conclusions Age, clinical course, and size of the lesion can be applied to distinguish MRT and RMPS. Five phenotypes have been identified and features of ulcers/protrusions should be further explored.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


